



Introduction
Rhabdomyolysis is a syndrome involving skeletal muscle damage caused by conditions such as severe trauma, physical exertion, seizure, drug use, toxins, biological agents, metabolic disorders, prolonged immobilization, and genetic defects. Subsequently, the breakdown of the damaged skeletal muscle leads to the release of its contents into plasma, thereby causing complications, such as acute kidney injury (AKI), electrolyte disturbance, compartment syndrome, and disseminated intravascular coagulation [1,2]. AKI is the leading cause of death in patients with rhabdomyolysis. Myoglobin-induced renal toxicity leads to rhabdomyolysis-associated AKI because of increased oxidative stress, inflammation, endothelial dysfunction, vasoconstriction, tubular obstruction, and apoptosis [1,3].
Rhabdomyolysis appears more frequently among male individuals, African-Americans, those aged younger than 10 or older than 60 years, and those with body mass index (BMI) values of greater than 40 kg/m2 [4]. However, the etiology of rhabdomyolysis and the incidence of AKI may vary depending on age [4–7]. Furthermore, large-scale multicenter studies on rhabdomyolysis and the associated risk factors for AKI in the pediatric population are scarce. The primary aim of this study was to investigate the characteristics of rhabdomyolysis in a Korean pediatric population. The secondary aim was to identify the risk factors for AKI among patients with rhabdomyolysis.
Methods
Study design
This retrospective study analyzed the medical records of children and adolescents diagnosed with and treated for rhabdomyolysis at 23 hospitals in South Korea from January 2007 to December 2016. This study was approved by the Institutional Review Board of Pusan National University School of Medicine and informed consent was waived due to the nature of the retrospective study (No. 05-2018-021).
Study population
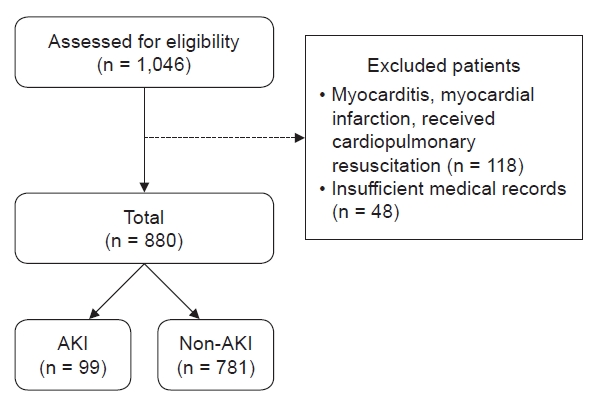
Rhabdomyolysis was defined by a creatine kinase (CK) level of at least 1,000 U/L or myoglobin level of at least 100 ng/mL. Patients eligible for inclusion were those aged between one month and 18 years who met the definition of having rhabdomyolysis (n = 1,046). Individuals were excluded from this study if they had myocarditis or myocardial infarction, had received cardiopulmonary resuscitation (n = 118) or had insufficient medical records (n = 48). Patients with muscular dystrophy were included only if they had not yet been diagnosed with such (n = 18). All subjects (n = 880) were divided into two AKI-status subgroups (with or without AKI) for comparison (Fig. 1).
Data collection
Medical records were reviewed to observe the following: age at diagnosis, sex, anthropometric data, symptoms, underlying illnesses, causal factors and complications of rhabdomyolysis, laboratory results, methods of treatment, and outcomes. All individuals were divided into five age subgroups because the incidence of rhabdomyolysis and the rate of AKI are not linearly associated with age [6]. Demographic data such as height, weight, and BMI were transformed into z-scores using the 2017 Korean National Growth Charts for Children and Adolescents (https://knhanes.cdc.go.kr/knhanes/sub08/sub08_02.do) and lambda–mu–sigma method [8]. AKI was defined as an increase in serum creatinine of at least 0.3 mg/dL within 48 hours or at least 1.5 times the minimum creatinine value during the hospitalized stay, regardless of the time period [9], which was established according to the creatinine criteria of the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines [10]. Oliguria was defined as a urine output of less than 0.5 mL/kg/hr for 12 hours. Urine output was determined based on details from the medical history, such as the time of last urination and medical records of urine output in the hospital. Multiorgan failure was defined as the failure of at least two of the major organ systems. Short-term and long-term outcomes were stratified based on a cutoff of 90 days after the date of AKI occurrence. The recovery duration of CK and myoglobin levels was defined as the period from the onset of rhabdomyolysis to the date of restoring the value in question to within the normal range. Volume overload was defined as the presence of pulmonary edema or peripheral edema. Chronic kidney disease was defined as a decrease in the glomerular filtration rate to less than 90 mL/min/1.73 m2, which was calculated using the updated Schwartz formula as follows: 0.413 × [height (cm)/serum creatinine (mg/dL)]. Laboratory parameters were analyzed by the following or equivalent methods: serum CK was analyzed by a CK N-acetyl-cystein-activated procedure; serum myoglobin was analyzed by chemiluminescence immunoassay; qualitative and quantitative urine myoglobin levels were analyzed by ammonia sulfate precipitation testing with urine test strips and electrochemiluminescence immunoassay, respectively; and serum creatinine was analyzed using the modified Jaffe’s kinetic method.
Statistical analysis
For the comparison of AKI and non-AKI subgroups, the Student t test or Mann-Whitney U test was performed for continuous variables, and the chi-squared test or Fisher exact test was performed for categorical variables. Multiple responses were allowed when surveying underlying diseases, causes, and complications of rhabdomyolysis. Statistical significance was set at p < 0.05.
We investigated whether AKI can be predicted by risk factors and initially accessible clinical information of patients with rhabdomyolysis. Multiple logistic regression analysis was performed to determine the independent risk factors associated with AKI. Candidate variables with p-values of less than 0.1 in the univariate analysis were entered into the model through variable selection by a stepwise method. Variance inflation factors were checked to eliminate multiple coherences. The results of the generated model were confirmed by the receiver-operating characteristic (ROC) curve and area under the ROC curve. All analyses were performed using R version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Demographic data and clinical symptoms
According to the study inclusion and exclusion criteria, 880 patients were included. The overall age distribution of these patients showed a bimodal peak (3–5 and 15–18 years, respectively). Among the five age subgroups, the largest one was those aged three to 5 years old in the total group and non-AKI subgroup, whereas it was 15 to 18 years old in the AKI subgroup. The median age at diagnosis was older in the AKI subgroup than in the non-AKI subgroup (12.2 years vs. 8.0 years; p < 0.001). There were 2.5 times more boys (ratio of boys:girls, 634:246), and all age subgroups were predominantly male (range of sex proportion, 2.0–3.6). Boys totaled 68.0% to 69.6% of patients younger than 12 years and 76.8% to 78.0% of those older than 12 years (Table 1).
Height, weight, and BMI z-scores did not significantly deviate from zero in the total rhabdomyolysis group. For those in the AKI subgroup, the actual height, weight, and BMI were higher, but their z-scores were not significantly different between the two subgroups. Body surface area was also higher in the AKI subgroup, but the z-scores could not be compared between the AKI-status subgroups because of a lack of data. Among the 880 patients, myalgia or muscle weakness was observed in 38.9% and dark-colored urine was present for 14.0%. Although oliguria occurred in only 4.1% of all rhabdomyolysis cases, it affected one-third of the AKI subgroup. Only 3.4% of all rhabdomyolysis cases had two or more causes of rhabdomyolysis. There were no significant differences in myalgia or muscle weakness, dark-colored urine, or the number of causal factors between the two AKI-status subgroups (Table 1).
Underlying disease
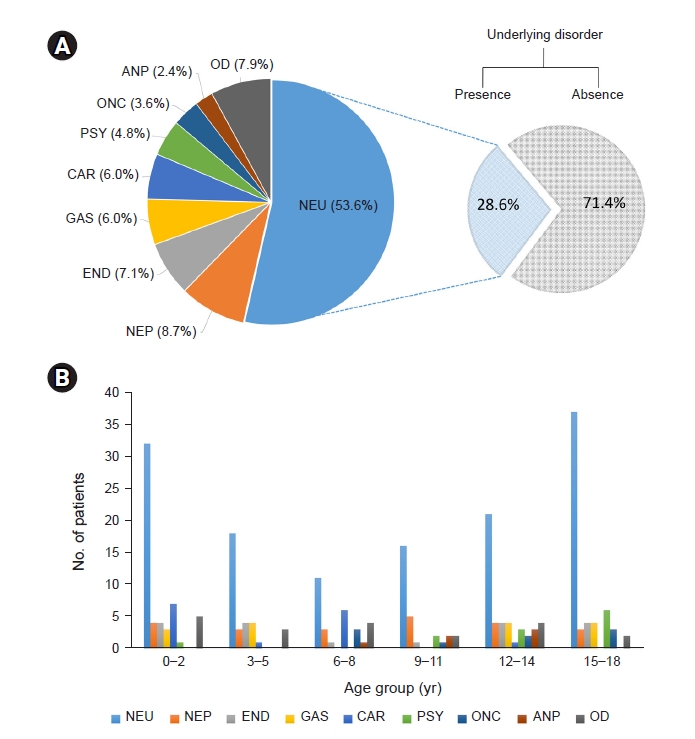
Of the 880 patients, 28.6% had underlying diseases. A detailed list of underlying disorders is provided in the supplementary data (Supplementary Table 1, available online). Neurological disorders were the most common underlying disorder (53.6%), followed by nephrological disorders, endocrinological and metabolic disorders, genetic and syndrome disorders, and cardiological disorders (Fig. 2A). The frequency of neurological disorders had a bimodal distribution and peaked in patients aged zero to 2 years and those aged 15 to 18 years, respectively. Most cardiological disorders were observed in patients younger than 9 years of age, whereas most psychiatric disorders were observed in those older than 9 years of age. No characteristic age distribution was identified for the other disorders (Fig. 2B). The underlying disorder that showed a significantly higher proportion in the AKI group included neurological disorders (26.3% vs. 14.0%; p = 0.002) and oncologic disorders (4.0% vs. 0.6%; p = 0.008). The proportion of total underlying disorders was higher in the AKI subgroup (53.5% vs. 25.5%; p < 0001).
Etiology
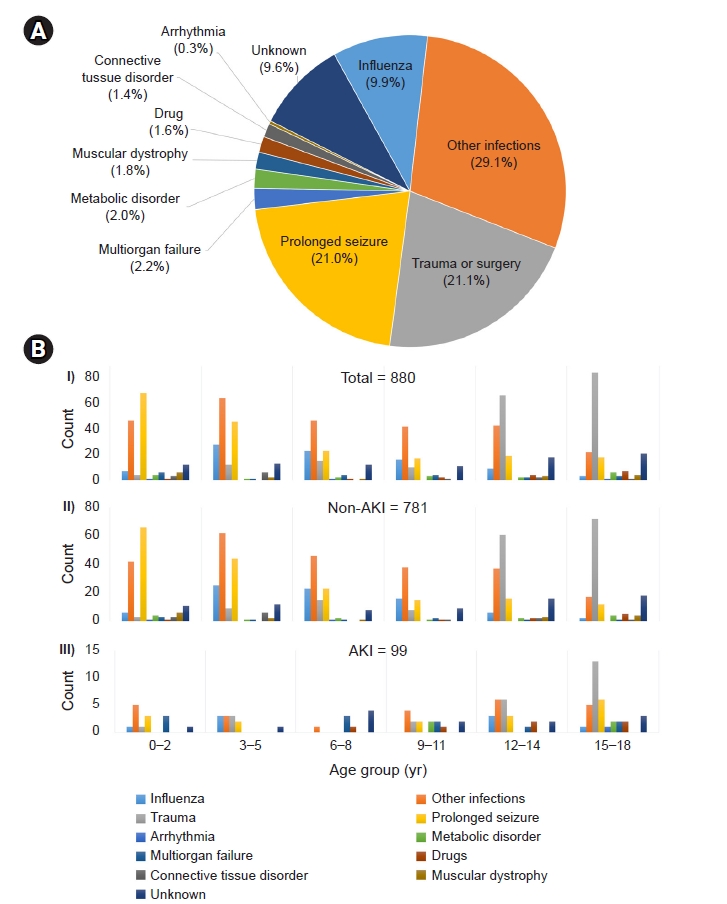
The most common cause of rhabdomyolysis was infection (39.0%), followed by trauma or surgery (21.1%), prolonged convulsions (21.0%), and unknown causes (9.6%). Other causes were diverse and heterogeneous, with a proportion of less than 3.0% (Fig. 3A). Influenza virus was the most common infectious cause. A detailed list of etiologies is shown in the supplementary data (Supplementary Table 2, available online).
Some causes of rhabdomyolysis were characterized by age; the greatest frequency of seizures and infections occurred at 0 to 2 years of age and 3 to 5 years of age, respectively. The frequency of trauma increased with age, with most cases occurring in patients aged 15 to 18 years (Fig. 3B-I). In the AKI group, although trauma was still prominent in older patients, the age pattern of infection and prolonged seizures in the total group became indistinctive. However, AKI was more frequently caused by relatively rare causes, such as drugs, multiorgan failure, cardiac arrhythmias, and metabolic disorders (Fig. 3B-II, III). Similarly, the differences in the frequency of infection (ratio of AKI:non-AKI subgroups, 36.0%:40.8%; p = 0.12) and prolonged seizure (18.1%:22.5%; p = 0.18) were not prominent, but those for multiorgan failure (12.4%:1.2%; p < 0.001) and drugs (6.7%:1.2%; p < 0.004) were significantly higher in the AKI subgroup.
Laboratory data
When the AKI and non-AKI subgroups were compared, most laboratory results showed significant differences between these two groups. A significantly greater proportion of AKI cases was associated with more positive urine occult blood (OB) (p < 0.001). The proportions of hematuria and urine myoglobin were higher in the AKI subgroup (p < 0.001 for both). Initial and peak CK and peak myoglobin levels were also significantly higher in the AKI subgroup, while the initial calcium levels were lower in the AKI subgroup. The initial and peak blood levels of parameters of interest, including aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), blood urea nitrogen (BUN), creatinine, uric acid, and phosphorus, were significantly higher in the AKI subgroup (Table 2).
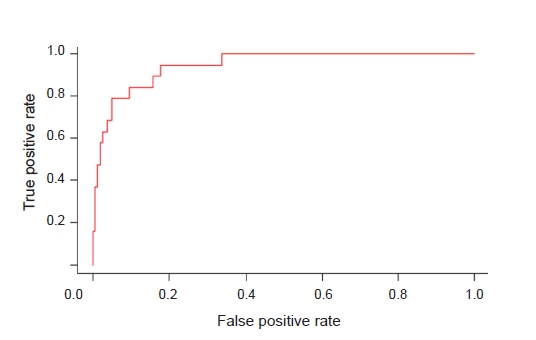
Among the results of univariate analysis (Table 1, 2), clinical information, which was initially assessable and whose p-value was less than 0.1, underwent stepwise variable selection, and the following variables were selected: age subgroup, the presence of underlying disease, multiorgan failure, urine OB, CK, AST, uric acid, calcium, and phosphorus. Based on the multiple logistic regression model for predicting AKI in rhabdomyolysis, variables that were independently associated with AKI development included the presence of underlying disease, multiorgan failure, urine OB, AST, uric acid, and calcium. Patients aged 15 to 18 years had an odds ratio of 2.3 relative to that of the reference group (3–5 years), but the p-value was insignificant. Urine OB 4+ and multiorgan failure-induced rhabdomyolysis had the highest odds ratios (Table 3). The discrimination value of the predictive model was established by means of an ROC curve, with an area under the ROC curve of 0.946 (p < 0.001) (Fig. 4).
Outcomes
CK and myoglobin were recovered within 5 to 6 days after the first day of rhabdomyolysis, and there was no difference between the AKI and non-AKI subgroups. Short-term outcomes in the AKI subgroup were characterized by a higher proportion of volume overload (33.8% vs. 0.7%; p < 0.001) and longer hospitalization (18 days vs. 6 days; p < 0.001). The median oliguria recovery time was 2.5 days in the AKI subgroup. The long-term outcomes of 522 patients, excluding those with missing data, revealed a greater proportion of chronic kidney disease and recurrent rhabdomyolysis in the AKI subgroup (p < 0.001) (Table 4).
Complications
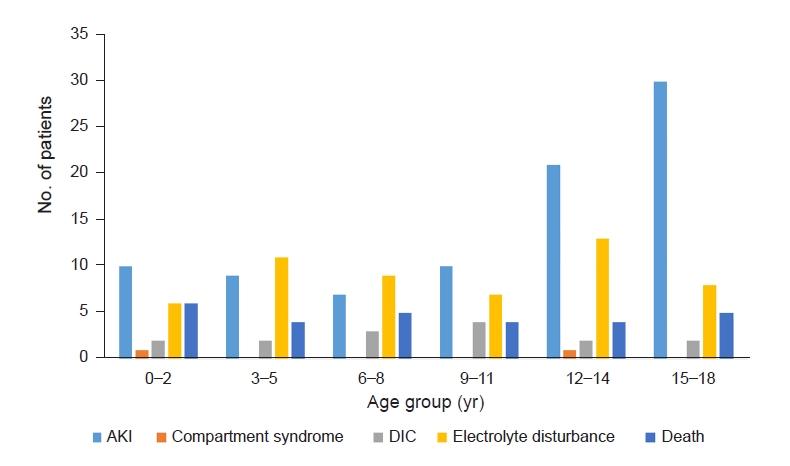
Only 15.4% of patients with rhabdomyolysis experienced complications. The total incidence of AKI was 11.3%; the incidence rates for the 0 to 9 years, 9 to 11 years, 12 to 14 years, and 15 to 18 years age subgroups were 6.4% to 7.9%, 11.3%, 13.4%, and 20.2%, respectively. The AKI subgroup presented a higher proportion of complications, such as mortality rate (14.1% vs. 1.8%), disseminated intravascular coagulation (12.1% vs. 0.4%), and electrolyte disturbance (25.3% vs. 3.7%) (Table 4, Fig. 5).
Treatment
In this study, 24.2% of patients did not require treatment, with a significantly higher proportion of these patients existing in the non-AKI group (p = 0.002). Volume replacement was the most commonly used treatment (72.1%). Alkalization and mannitol administration were performed significantly more often in the AKI subgroup (p < 0.001). Dialysis was performed in 31.3% of the 99 patients with AKI. Peritoneal dialysis was performed in only one patient, while the others required continuous renal replacement therapy (CRRT) (Table 5). The average dialysis period was 10.6 days.
Discussion
Rhabdomyolysis has been defined in various ways in previous studies. A CK level of at least 1,000 U/L or exceeding 5 times the upper limit of the normal range has been commonly used as the cutoff value for diagnosis [4], but those of at least 5,000 U/L and at least 10,000 U/L have also been adopted [8–10]. Another criterion that is less frequently used is myoglobin, whose reference level in previous studies ranged from at least 80 ng/mL to at least 150 ng/mL [7,11,12]. We used either CK or myoglobin level as the inclusion criteria for our study to maximize the number of participants.
Because of the diversity of definitions and subjects, the incidence of rhabdomyolysis varies from 4% to 50% in adult studies [3,11]. The exact incidence of pediatric rhabdomyolysis is unclear, but it has been reported to range from 5% to 37.5% [5–7]. Approximately 4% to 50% of cases of rhabdomyolysis lead to AKI, while up to 15% of AKI cases can be attributed to rhabdomyolysis [1–3]. The incidence of AKI in our study was 11.3%. We believe that the use of a single, universal definition of rhabdomyolysis is necessary because it will aid in comparing incidence rates between studies and lead to advancements in this field.
A pediatric study performed in Korea investigated rhabdomyolysis in 39 children and reported the findings of a higher proportion of boys (2.5-fold more) among the affected children, epilepsy as the most common underlying disorder, and infection as the most common cause, similar to our results [7]. Another pediatric study that involved 172 children in Taiwan reported the existence of a higher proportion of boys (3.7-fold more) among the total cases and found viral myositis to be the most common cause. However, these authors also reported an absence of sex differences in AKI incidence [6]. Similarly, our study also revealed a male sex dominance. The higher proportion of adolescent males in rhabdomyolysis cases suggests that sex hormones or greater physical activity, which leads to more muscle mass, may contribute to the development of rhabdomyolysis. There were no sex differences in the proportion of causes, underlying disease, or complications of rhabdomyolysis in our study. Further studies are needed to determine whether sex contributes to rhabdomyolysis. We also did not observe any differences in the incidence of AKI according to sex. Therefore, male sex is not a risk factor for rhabdomyolysis-induced AKI.
The influence of anthropometric data on rhabdomyolysis and AKI has not been fully elucidated, and reports on the association between rhabdomyolysis and obesity are limited. Increased BMI could reflect a large muscle mass but usually implies excess adipose tissue that could induce pathological changes in the kidney and increase baseline circulating levels of nephrotoxic inflammatory molecules [13]. Several adult studies have indicated that obesity and high BMI are linked to rhabdomyolysis and AKI [14–17]. In a single-center cohort study on obesity and AKI unrelated to rhabdomyolysis, obese patients were more likely to develop AKI, and each 5-kg/m2 increase in BMI was associated with a 10% greater risk of severe AKI [14]. However, BMI was not associated with AKI in a previous pediatric study [6], and the z-scores of height, weight, and BMI did not differ between the AKI and non-AKI subgroups in our study. At this time, the reason why there is a contradiction regarding the influence of obesity on rhabdomyolysis and AKI between adults and children remains unclear. With respect to the different results between pediatric and adult studies, limitations of BMI, body composition, and duration of obesity might affect the risk of AKI.
Although myalgia, weakness, and dark-colored urine have been known as the classic triad of symptoms of rhabdomyolysis, these findings are observed in less than 10% of affected patients. In a previous report, more than 50% of patients did not have myalgia or weakness, while dark-colored urine was observed in only 3.6% of the cases [2]. Our cases showed a relatively greater proportion of the classic triad than found in previous studies, but these symptoms were not distinguishing features of the AKI subgroup.
It is well known that infants and toddlers are vulnerable to febrile illness and seizures and that outside activities and accidents tend to increase in adolescents. The etiologic distribution of bimodal distribution in our study reflects these characteristics and may influence the frequency of rhabdomyolysis in each age group. Therefore, these etiological results vary depending upon the subpopulation. Previous adult studies suggested that trauma and illicit drug abuse are primary causes of rhabdomyolysis [18–20]. In our study, trauma was the second most common cause of rhabdomyolysis and was more prevalent in adolescent patients. However, drug-induced rhabdomyolysis accounted for only 1.7% of cases, and there were no cases of illicit drug use. Relatively low frequencies of trauma-induced and drug-induced rhabdomyolysis are believed to reflect the characteristics of the pediatric population and low prevalence of drug abuse in Korea [21,22]. Therefore, we suggest that the causes of rhabdomyolysis should be investigated in specific subpopulations.
Patients who experience seizures are considered vulnerable to rhabdomyolysis for two reasons. First, seizures lead to postictal alterations in several blood parameters, such as CK [23]. It is well known that skeletal muscle injury can be caused by convulsive seizures or status epilepticus [24]. Second, the majority of antiepileptic drugs, such as valproic acid and levetiracetam, are relevant to rhabdomyolysis [25]. Some neuromuscular disorders, such as muscular dystrophy, are accompanied by increased CK levels, which are susceptible to triggering factors such as fever, exercise, bisphosphonate use, and anesthesia [26–28]. A retrospective study reported 13 patients with rhabdomyolysis featuring muscular dystrophy; the median duration between the first episodes of rhabdomyolysis and genetic diagnosis was 2 years, and the authors suggested that persistently increased CK levels with recurrent rhabdomyolysis warrant a workup for underlying muscular dystrophy [28].
Muscle-derived components are effective biomarkers for renal damage, resulting in hyperphosphatemia; hypocalcemia; hyperuricemia; increased plasma LDH and AST levels; and increased urinary excretion of creatinine, uric acid, and glucose [29]. Although CK is a cornerstone of rhabdomyolysis diagnosis, it remains controversial whether CK itself is related to the risk of AKI and mortality. Some studies have shown that the initial or peak CK value is not a reliable marker of AKI or mortality outcome [30–32]. However, other studies have suggested that the initial and peak values of CK and myoglobin are risk factors for AKI [6,20]. Our study showed that the initial CK level was significantly increased, but that of myoglobin was not. These contradictory results regarding CK and myoglobin may be affected by differences in the time interval from symptom onset to arrival at the hospital. CK levels rise in rhabdomyolysis within 12 hours of the onset of muscle injury, peak within 24 to 72 hours, and normalize approximately 5 days after the cessation of muscle injury. The half-life of CK is approximately 36 hours [33]. Meanwhile, myoglobin has a short half-life (2–4 hours) and may return to normal within 6 to 8 hours [2]. In future studies, it is worth considering adjusting the initial CK level according to the timing of muscle injury.
Our study revealed significant differences in most traditional biomarkers, including AST, ALT, LDH, uric acid, calcium, and phosphorus. Although they were not included in our study, constant albuminuria and hypoalbuminemia have been suggested as independent risk factors for AKI in previous research [7,20]. In this respect, timely measurements of traditional biomarkers are useful and practical for predicting AKI. The McMahon score predicts the risk of renal failure requiring renal replacement therapy (RRT) or resulting in mortality in patients with rhabdomyolysis. The variables include age; female sex; origin of rhabdomyolysis; and initial values of creatinine, calcium, CK, and phosphate. A McMahon score of 6 points or higher has greater sensitivity and specificity than a CK level of greater than 5,000 U/L in predicting the risk of RRT [34]. Although the McMahon score was developed for adult patients, modification of variables based on our and other pediatric studies may give us a scoring system applicable to children in future studies.
Dipstick urine OB can yield false-positive results caused by dehydration, exercise, hemoglobinuria, and myoglobinuria, which are commonly seen in rhabdomyolysis [1,35]. However, it is an inexpensive and rapid test that is useful for detecting the risk-estimation markers of AKI. The correlation between AKI and urine OB shown in our study supports the usefulness of the urine dipstick test. In our study, dark-colored urine did not show any difference between the AKI-status subgroups, while true hematuria was significantly higher in the AKI subgroup. Thus, the influence of hematuria on the degree of urine OB is greater than that of myoglobin in this group, and these results suggest a role of hematuria in AKI. Hematuria has a pathophysiological mechanism that is involved in aspects of renal damage, such as direct tubular damage, oxidative stress, and secretion of inflammatory cytokines, which occurs during rhabdomyolysis [36]. Hematuria is presumed to aggravate kidney function in patients with rhabdomyolysis. Therefore, the risk of AKI could increase in cases of true hematuria and patients with higher OB scores following urinalysis.
Fluid resuscitation has been widely used to treat rhabdomyolysis, and it was also the most commonly used method in our study. Although fluid therapy is emphasized by consensus [5,37,38], other treatment methods are still controversial. Dawley [37] reported that management consists of rapidly aggressive intravenous resuscitation to maintain urine output and limited use of bicarbonate for acidosis and mannitol for oliguria, respectively. Michelsen et al. [38] reported guidelines that recommend early fluid resuscitation using crystalloids but not the routine use of diuretics, mannitol, alkalization, or RRT. CRRT effectively removes myoglobin and manages AKI [38]. A Cochrane systematic review concluded that CRRT provides some benefits, but the evidence is insufficient [39]. However, significantly decreased myoglobin levels; improved BUN, creatinine, and potassium levels; and reduced oliguria and hospitalizations were reported relative to when conventional therapy was used. Mortality rates exhibited significant differences, but data on long-term outcomes are lacking [39].
To our knowledge, this is the first large-scale pediatric multicenter study. First, our study clarified the age distribution, proportions of boys and girls, and anthropometric data in rhabdomyolysis, which have been reported in previous studies. Second, our detailing of underlying diseases and causes of rhabdomyolysis can help in understanding their influence in the pediatric population. Third, we found that the independent risk factors for AKI in rhabdomyolysis were multiorgan failure; the presence of underlying disorders; increased levels of urine OB, AST, and uric acid; and decreased levels of calcium. Unlike in previous adult studies, sex, BMI, and CK were not included as risk factors. Fourth, the role of urinalysis was newly highlighted for predicting AKI.
However, there are some limitations to account for as this was a retrospective multicenter study. First, some medical record data regarding etiology, underlying disorders, and laboratory data were missing, which led to the exclusion of some cases. Second, AKI and oliguria could be underestimated or overestimated because of the methodological issues with baseline creatinine level and urine output. Third, some laboratory data, such as CK and myoglobin levels and urine red blood cell count exceeding the upper reference limit, were reported only as values over the upper limit instead of the exact value, which might have led to underestimation of their influence. In addition, the analysis methods and equipment used likely varied among the involved hospitals. Fourth, underlying disorders were classified based on the involved organ or pathology of the disease for the purpose of detailed descriptions, but the criteria for classification were vague for disorders with multisystemic involvement, and severity was not considered. Thus, the interpretation of the influence of underlying disorders on rhabdomyolysis and AKI is limited.
Rhabdomyolysis is a well-known disease, but its epidemiology, risk factors, incidence rates of AKI, and mortality have not been elucidated because of the heterogeneity caused by varying definitions and etiologies. Our study revealed characteristic clinical and laboratory features of rhabdomyolysis in a multicenter Korean pediatric population as well as the predictive factors for AKI. These findings will contribute to a broader understanding of pediatric rhabdomyolysis and enable early intervention against rhabdomyolysis-induced AKI.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









