



Introduction
The severe acute respiratory syndrome coronavirus 2 or coronavirus disease 2019 (COVID-19) pandemic has caused unprecedented threats to public health, disproportionally against the old and those with underlying health conditions. As the incidence rate of COVID-19 has increased exponentially, social distancing and the use of personal protective equipment (PPE) have been recommended and often enforced worldwide. Social distancing measures range from strict nationwide lockdown and/or curfew to more voluntary-based recommendations. In countries such as South Korea, varying stages of social (or physical) distancing measures were implemented depending on the extent of the viral spread in combination with rapid screening and efficient contact tracing without imposing draconian ŌĆśstay-at-homeŌĆÖ restrictions [1ŌĆō3]. Regardless of the extent of legal enforcement, the common factors in social distancing include avoidance of contact with other people, hygienic behavior, and the use of PPE.
Chronic kidney disease (CKD) is a common health problem worldwide, with a global prevalence reaching 29.3% in 2017 [4]. CKD is not only recognized as a risk factor for infectious diseases but may also aggravate their prognosis [5ŌĆō7]. Indeed, CKD patients exhibit a significantly higher fatality rate following COVID-19 infection than the general population [8]. It is necessary to protect CKD patients from potential COVID-19 infection. Hence, health practitioners and clinicians need to understand the current status of compliance with precautionary recommendations among CKD patients, and the factors that influence their precautionary behaviors.
While active social distancing measures have contributed to a decrease in new cases by reducing the likelihood of transmitting COVID-19, these measures may lead to undesirable consequences, including physical inactivity. Recent initial reports indicate that the stay-at-home orders in several countries caused significant decreases in physical activity not only among general or healthy populations but also among patients who require routine physical exercise [9,10]. Physical inactivity is responsible for approximately 3.2 million deaths per year [11]. Moreover, for CKD patients, a lack of physical activity has often been linked to adverse prognoses [12ŌĆō14]. For this reason, we evaluate the impact of behavioral change on the physical activity of CKD patients.
This study was conducted to determine the current status of precautionary behaviors against the COVID-19 pandemic among CKD patients along with their physical activity during the first months of the pandemic. The observations made in this study can help to develop the most appropriate clinical recommendations in this vulnerable population to prevent COVID-19 infection and to promote healthy behavior that will improve the maintenance of underlying disease.
Methods
Study populations
This study was conducted with a cohort of CKD patients. The Study on Kidney Disease and Environmental Chemicals (SKETCH, Clinical Trial No. NCT04679168) aims to investigate the behavioral characteristics, chemical exposure, and clinical outcomes of CKD patients during and after the COVID-19 pandemic. We defined CKD as (1) estimated glomerular filtration rate (eGFR) of Ōēź15 and <60 mL/min/1.73 m2 or (2) eGFR of Ōēź60 mL/min/1.73 m2 and urine protein to creatinine ratio of >0.3 g/g. A total of 308 participants were recruited from five university hospitals located in Seoul, Ilsan, and Daegu, Korea between June and October 2020 (Supplementary Fig. 1, available online). Exclusion criteria included those who were followed up less than 3 months or with a recent history of acute kidney injury, progressive malignancy, cerebral infarction, cerebral hemorrhage, myocardial infarction, under hemodialysis, or immunosuppressant use.
The study protocol and consent to participate were approved by the Institutional Review Board in participating hospitals (Supplementary data 1, available online). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Questionnaire and clinical data
A questionnaire survey was conducted by trained surveyors for participating patients on their visit to the hospital. The questionnaire included questions related to 1) risk perception of COVID-19, 2) hygienic behavior, 3) social distancing, and 4) physical activity during the past year (before the pandemic) and the 1 month before the hospital visit (during the pandemic). Detailed information of the survey was described in Supplementary data 2 (available online). Perceived risk of COVID-19 infection was determined by a 5-point scale from ŌĆśneverŌĆÖ (1) to ŌĆśextremely highŌĆÖ (5); items, marked 4 or 5 were grouped as high-risk perception or ŌĆśhigh perceived risk.ŌĆÖ For evaluating the risk perception among the general population of Korea, the relevant data (i.e., the possibility of personal COVID-19 infection) was gleaned from Hankook Research (https://hrcopinion.co.kr/covid-19, accessed December 18, 2020) which collected data from 1,000 subjects through biweekly survey events. The statistics for the incidence of COVID-19 infection were obtained from the Korean Statistical Information Service (https://kosis.kr/covid/covid_index.do, accessed December 13, 2020).
Demographic data, anthropometric data, and clinical laboratory data related to CKD were obtained when the subject visited the hospital (Supplementary data 3, available online). Data on underlying comorbidities were collected via electronic medical records using prescription records and diagnostic codes according to the International Classification of Diseases 10th Revision (ICD-10).
Statistical analysis
The chi-square tests and Fisher exact tests for categorical variables were conducted to compare demographic and clinical parameters by CKD status. In addition, the Mann-Whitney U test and the Student t test were performed for continuous variables. Categorical variables were expressed as numerical with proportions (%), and continuous variables were expressed as mean ┬▒ standard deviation when distributed normally (as median with interquartile range otherwise).
To compare behaviors before and during the COVID-19 pandemic, the Wilcoxon signed-rank test was used. Logistic regression analysis was conducted to identify the relative factors related to risk recognition or behavior changes. Sensitivity analysis was conducted with age adjustment because the odds ratio (OR) of high-degree perception was greater than scale ŌĆś3ŌĆÖ in the groups aged Ōēź60 years. First, we assessed the associations between possible demographic factors and risk recognition following stratification by age group (<60 years, Ōēź60 years). Second, the age group (1, <50 years; 2, 50ŌĆō59 years; 3, 60ŌĆō69 years; and 4: Ōēź70 years) was additionally adjusted as a covariate in logistic regression models. The p values of <0.05 were defined as significant when they were set to two-sided. Statistical analyses were performed using IBM SPSS version 23.0 (IBM Corp., Armonk, NY, USA) and SAS version 9.4 (SAS Institute, Cary, NC, USA). Spearman correlation was visualized by using the package corrplot (R 3.5.3; R Foundation for Statistical Computing, Vienna, Austria).
Results
Study populations
The mean age of the participating CKD patients (n = 306) was 61.0 ┬▒ 12.5 years, and 209 patients (68.3%) were male (Table 1). The mean serum creatinine and eGFR of the patients were 1.8 ┬▒ 0.7 mg/dL and 43.2 ┬▒ 20.7 mL/min/1.73 m2, respectively. A total of 187 patients (61.1%) showed an eGFR less than 45 mL/min/1.73 m2 and were regarded as the advanced CKD group. Advanced CKD was found more frequently among older and female patients; these patients tended to show lower serum hemoglobin, platelet, serum albumin, bilirubin, and a higher proportion of overt proteinuria (Table 1).
The majority of patients had completed a high school education (35.9%) or higher (29.2%). A total of 137 participants (44.8%) were working either full or part-time. There were 56 (18.3%) and 85 participants (27.8%) with current smoking and alcohol consumption, respectively. Most participating CKD patients stated their health status as ŌĆśnot goodŌĆÖ (43.1%) or ŌĆśbadŌĆÖ (46.7%).
Risk perception
At the time of the survey during the global pandemic of COVID-19, in general, most participating patients (89%) perceived the risk of infection as ŌĆśserious.ŌĆÖ More people considered the general risk of infection nationwide (i.e., ŌĆśnationwide in generalŌĆÖ) as serious (76.1%) than the risk for their city of residence (55.4%) or the individual (45.6%) (Supplementary Fig. 2, available online).
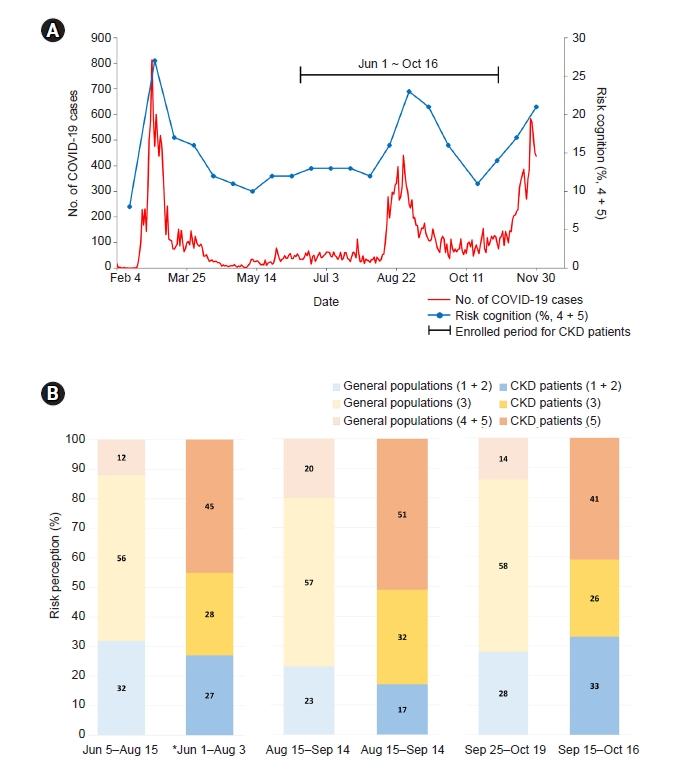
In CKD patients, risk perception for the city of residence or the individual was also significantly correlated with trends of COVID-19 case reporting (Supplementary Table 1, available online). Based on this result, we used the risk perception variable as the risk on the individuals to evaluate the impact on behavior changes. The level of perceived risk in general populations appeared to be related to the trends in cases of COVID-19 infection (Fig. 1A). Most patients of the cohort were enrolled after the first peak of the pandemic. Compared to the general population of Korea (n = 1,000), CKD patients showed much greater levels of the perceived risk from COVID-19 infection (Fig. 1B).
Older patients with lower education and income were more likely to perceive a greater risk of infection. The stage of CKD, however, did not influence the risk perception (Table 2). When stratified by age group, the associations of education and income with risk perception disappeared (Supplementary Table 2, available online).
Behavioral changes during the COVID-19 pandemic
The frequencies of ŌĆśpublic transport useŌĆÖ and ŌĆśpublic place visitŌĆÖ were significantly decreased in all populations regardless of the frequency of such behaviors before the pandemic (Table 3). The frequency of ŌĆśprivate vehicle useŌĆÖ tended to increase among those who seldom used private transport before the pandemic, but among those who frequently used private vehicles, the frequency of use decreased (Supplementary Fig. 3A, available online).
During the pandemic, CKD patients showed significant increases in several hygiene-related behaviors. The frequency of handwashing, showering, face mask use, and hand sanitizer use was significantly increased during the COVID-19 pandemic. In particular, there were no subjects who did not wear a face mask during the pandemic (p < 0.001). In addition, the frequencies of laundry and house cleaning were significantly increased (p < 0.001) (Supplementary Fig. 3B).
Regarding the frequency of exercise, i.e., physical activity over 30 minutes, no change was observed in general (n = 306) and in those who exercised on an irregular basis (n = 128). Among those who exercised regularly (n = 178) or in gyms (n = 28), however, the frequency of exercise significantly decreased.
Factors associated with social distancing behaviors
Several demographic and socioeconomic factors were associated with behaviors related to social distancing (Table 4). Younger patients (<50 years old) showed less frequent public place visits and more exercise. Patients with higher income showed >1.5 ORs for less frequent public place visits and longer stays-at-home (Supplementary Table 3, available online). The positive associations of stay-at-home with sex and income became stronger after age adjustment (Table 4).
Higher risk perception was significantly associated with decreased use of public transport (OR, 2.00; 95% CI, 1.09ŌĆō3.66), and the association remained significant after adjustment for age (adjusted OR, 1.91; 95% CI, 1.01ŌĆō3.60) (Table 4). Among patients with diabetes, the negative association with the frequency of public place visits was attenuated by age adjustment (adjusted OR, 0.66; 95% CI, 0.41ŌĆō1.05). In addition, advanced CKD patients tended to stay-at-home for shorter times even after adjusting for age (adjusted OR, 0.54; 95% CI, 0.33ŌĆō0.88) (Table 4).
Factors associated with hygiene-related behaviors
Behaviors related to personal hygiene were related to age, education, and CKD stage, even though clear linearities were often unseen (Supplementary Table 4, available online). Hand sanitizer use was more frequent among people with higher education and higher income (Table 5). In addition, patients with higher income tended to perform laundry and house cleaning more frequently. The positive association between income and frequency of laundry remained significant after age adjustment (Table 5). The frequencies of handwashing and face mask use, however, were not influenced by any factors assessed in the present study.
The level of risk perception was not related to hygiene-related behaviors. In addition, CCI status was not associated with hygienic behaviors except for hand sanitizer use (Table 5). However, among patients with diabetes, the use of hand sanitizer was significantly decreased (OR, 0.47; 95% CI, 0.23ŌĆō0.99), and the number of clothes used between laundering was significantly increased (OR, 0.46; 95% CI, 0.21ŌĆō0.97) compared to non-diabetes patients even after adjustment for age (Table 5). Advanced CKD status showed a significant association only with the decreased frequency of showering (OR, 0.52; 95% CI, 0.29ŌĆō0.93).
Factors associated with physical activities
In general, exercise behavior among CKD patients was not affected during the COVID-19 pandemic. Among those who had exercised regularly, the frequency of exercise was negatively associated with age (OR, 0.26; 95% CI, 0.09ŌĆō0.74). Among those who took regular exercise, education (OR, 5.47; 95% CI, 1.22ŌĆō24.62) and income (OR, 6.59; 95% CI, 1.84ŌĆō23.68) status were positively associated with exercise (Supplementary Table 5, available online). The positive association of income remained significant even after adjustment for age in patients who took regular exercise (Table 6).
Discussion
Among the participating patients with CKD, the COVID-19 pandemic significantly altered behavioral characteristics related to social distancing, hygiene, and physical activity. Since the outbreak of the COVID-19 pandemic, several observations on behavioral changes among chronic disease patients have been reported [15,16]; however, no reports have been made on CKD patients. Because such behavioral changes may influence the progress or prognosis of underlying diseases, including CKD and also COVID-19 infection, characterizing behavioral changes in patients has important clinical implications [5,6,8].
The participating patients with CKD showed a greater level of risk perception toward COVID-19 infection, i.e., >2 times greater proportion of the SKETCH cohort answered ŌĆśseriousŌĆÖ or ŌĆśvery seriousŌĆÖ for the possibility of COVID-19 infection risk, compared to the general population of Korea. Several hygienic behaviors were also more frequently adopted among CKD patients than the general Korean population, for example, the use of face masks (100% vs. 63.2% in the general population) and hand hygiene (93.7% vs. 67.8% in the general population) during the first wave of the pandemic (February 2020) [17]. Risk perception is generally considered to be related to culture, worldview, experience, and prosocial values and is often amplified through friends and family [18]. The higher perceived risk of infection among the participating CKD patients may be partly due to the underlying disease; comorbidities were suggested as one key indicator that could increase the perception of risk [19].
Socioeconomic status including education, income (higher), and sex (female) are negatively correlated with unhealthy behaviors [20,21]. In addition, the severity of comorbidities is closely related to the tendency toward healthy behavior. Patients with more comorbidities tend to engage in more conservative behaviors for the sake of their health [22]. In United States adults (n = 6,463) from March to April 2020, hygiene-related behaviors such as handwashing and surface disinfection were more common among females and those older patients with higher income, higher education, and self-rated good health [21]. Except for self-rated health status, these findings are generally comparable to the observations made for the present CKD patients. Longer stay-at-home behavior among CKD patients may reflect higher levels of risk perception among these patients in comparison to the general population of Korea (Fig. 1B). Although the stage of CKD was inversely associated with increased stay-at-home time, it might be related to a discrepancy between risk perception and behavior change due to the worse socioeconomic and education status in advanced CKD patients.
The lack of significant changes in the frequencies of handwashing and face mask use by key socioeconomic factors such as education and income warrant further discussion because these factors have been recognized as drivers of healthy or conservative behaviors. Null associations with handwashing and face mask use remained the same regardless of age adjustment (Table 5). These observations can be explained by the almost unanimous use of face masks (100%) and much greater frequency of handwashing (86.3% vs. 67.8% among the general population [17]) in the present CKD patients regardless of socioeconomic status or sex.
Stringent social distancing or self-isolation may produce side effects such as physical inactivity, which may lead to other health issues [23]. In the United Kingdom, the prevalence of physical activity was found to be substantially lower in general among adults than before the pandemic, and this change was attributed to the requirement for self-isolation and stay-at-home orders [24]. Moreover, patients with comorbidities tended to be less physically active during the pandemic than the matching healthy population [25,26]. Unlike previous studies that reported notable decreases in physical activity, our findings showed that the physical activity of CKD patients in Korea was generally unaffected during the COVID-19 pandemic (Supplementary Fig. 3C). These observations indicate the target population to whom clinical recommendations for exercise should be delivered.
Physical activity is an important component in the management of kidney disease; it helps to reduce inflammation, improve glomerular filtration rate, and reduce albuminuria [12ŌĆō14] and is often related to the quality of life in CKD patients [27]. Guidelines for adequate levels of exercise are therefore warranted for CKD patients, especially during the pandemic, which has led to reduced physical activities. One survey of patients with kidney transplantation in Germany showed that a telemedicine-based aftercare program could efficiently increase overall activity during the COVID-19 pandemic, although sports activities decreased [28]. This interesting observation may be attributable not only to an effective follow-up care program but also to the less strict social distancing policy of Germany that allowed outdoor physical activity [28]. Follow-up and intervention programs designed specifically for CKD patients to maintain or enhance physical activity are recommended for this vulnerable population during the pandemic when self-isolation is involved.
This study is the first report of the behavioral characteristics and changes among CKD patients during the COVID-19 pandemic in Korea. As a cross-sectional study of a group of CKD patients recruited via convenience sampling, the observations of this study may not be generalizable. In addition, there are limitations for exact comparison to general populations because of the restriction on the population with CKD. Finally, because of the structural limitations for reflecting the different baseline characteristics between the subgroups in the logistic regression analysis, ordinary concepts were not applicable in some of the results. Despite presenting only a snapshot observation on CKD patients during this global pandemic, the results of this study can help health practitioners design relevant recommendations for CKD patients not only to reduce the likelihood of COVID-19 infection but also to maintain health-related behaviors.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









