


Introduction
Among critically ill patients admitted to intensive care units (ICUs), acute kidney injury (AKI) is observed in 15% to 60% [1–5] and is associated with increased risks for a longer ICU or hospital stay, ICU or in-hospital mortality, and chronic kidney disease (CKD) progression [6–8]. Despite recent technical advancements in kidney-supporting devices [9–12], mortality from AKI remains high. This may be due to multiple factors, such as increased illness severity, variation in AKI phenotype, and delayed recognition of AKI [13–16], resulting in delayed nephrology consultation and management [17,18].
Since the early 2000s, the importance of timely nephrology consultation for critically ill patients with AKI has been studied in several countries. In 2002, Mehta et al. [17] evaluated ICU patients in four teaching hospitals in the United States and found that in-hospital mortality was higher and the length of ICU stay was longer in patients with delayed (>48 hours after AKI onset) nephrology consultation. In a retrospective observational study conducted at a Brazilian teaching hospital published in 2011, patients evaluated by nephrologists were more seriously ill than those not evaluated by nephrologists, although the ICU mortality rates were similar [18].
The involvement of nephrologists in the management of ICU patients depends on the nation or time period. Over the past 10 years, multiple randomized controlled trials of renal-replacement therapy (RRT) [19–22] have been conducted, leading to increased awareness among non-nephrology intensivists regarding the importance of early detection of AKI and timely dialysis [23,24]. Increased availability of continuous RRT (CRRT) machines has also made it easier to access RRT in the ICU [25] compared to the early 2000s. Therefore, the role of early nephrology consultation is unclear at this moment. Furthermore, the effect of nephrology consultation on the outcomes of critically ill AKI patients has rarely been evaluated in South Korea.
In this study, we examined the effectiveness of nephrology consultation in AKI patients by analyzing data for the period 2011 to 2020 extracted from the electronic medical records (EMR) of two tertiary teaching hospitals in South Korea.
Methods
The Institutional Review Board (IRB) of Pusan National University Hospital approved the study protocol (No. 2306-023-128), and the IRB waived the requirement for informed consent (consent for publication: not applicable).
Design and setting
This was a multicenter, retrospective cohort study of critically ill patients admitted to two tertiary teaching hospitals in South Korea. We included adult (age, >18 years) patients admitted to six ICUs (medial, pulmonary, surgical, trauma, neurosurgery, and emergency ICUs) in Pusan National University Hospital and Pusan National University Yangsan Hospital between January 2011 and December 2020. We excluded patients with end-stage kidney disease undergoing maintenance dialysis, those with missing serum creatinine data, and those admitted to nephrology department. We extracted patient data from EMRs. Excluding CKD, comorbidities were identified based on the International Classification of Diseases, 10th revision (ICD-10) codes and the medications prescribed. CKD was defined based on estimated glomerular filtration rates measured between 1 year and 3 months before hospital admission, in addition to ICD-10 codes (Supplementary Table 1, available online). We extracted departmental information for each patient to categorize patients as medical or surgical (Supplementary Fig. 1, available online).
Detection of acute kidney injury and nephrology consultation
AKI during the ICU stay was detected retrospectively based on the KDIGO serum creatinine criteria of an increase in the serum level of creatinine of ≥0.3 mg/dL within 48 hours [26]. Resolving AKI was also retrospectively defined as the decrease in serum creatinine level of ≥0.3 mg/dL within 48 hours [27–29]. The urine output criterion was ignored. The AKI diagnosis date was defined as the first day on which a significant change in serum creatinine level was detected. The peak AKI stage was calculated based on the highest serum creatinine level after detection of AKI; stages 1, 2, and 3 were defined as 1.5- to 2-fold, 2- to 3-fold, and >3-fold increases from baseline [26]. The decision to initiate dialysis was at the discretion of attending physicians. Dialysis information was extracted from the EMRs using a procedural code; all cases of AKI with dialysis were staged as 3D.
Nephrology consultations during the ICU stay were retrieved from the EMRs. We defined early nephrology consultations as those occurring within 48 hours after the onset of AKI, and delayed nephrology consultations as those occurring 48 hours or more after the onset of AKI.
We retrospectively calculated the sequential organ failure assessment (SOFA) scores at ICU admission [30]. Systemic inflammatory response syndrome (SIRS) was identified if two or more of the following criteria were met: body temperature, > 38 ℃ or <36 ℃; heart rate, >90 beats/min; respiratory rate, >20 breaths/min; and leukocyte count, >12 × 109 or <4 × 109/L [31].
Statistical analysis
We checked data normality using the Kolmogorov-Smirnov test. Continuous variables are expressed as medians with interquartile ranges (IQRs) or means ± standard deviations (SDs), as appropriate. Differences between the two groups were compared using the Student t test. Categorical variables are expressed as percentages, and proportions were compared employing the chi-square test.
The effects of nephrology consultation on in-hospital mortality were analyzed via univariable and multivariable Cox proportional hazards models. The full model was adjusted for age, sex, diabetes and hypertension status, CKD status, stroke, cancer, SOFA score, sepsis, AKI stage, serum level of albumin, and heart-, lung-, and liver-disease status. For the final model, backward selection was used based on the Wald test with a threshold of 0.2 for all predictors. The Kaplan-Meier survival curves and regression plots were used to compare the effects of nephrology consultation among AKI subgroups. All statistical tests were two-sided, and p-values of <0.05 were considered significant. Data were analyzed and plotted using IBM SPSS software (ver. 29.0; IBM Corp.).
Results
Baseline characteristics
In total, 2,416 AKI patients were included. The median age was 65 years (IQR, 56–75 years), 1,459 (59.3%) were male, 1,399 (56.8%) had diabetes, 985 (40%) had cancer, and 784 (31.9%) had CKD before ICU admission. At ICU admission, 1,132 (46.0%) had sepsis, and the mean ± SD of SOFA score was 7.89 ± 3.69. Of the 2,416 AKI patients, 915 (37.2%) were stage 1, 481 (19.5%) were stage 2, and 1,065 (43.3%) were stage 3 at the peak. During the ICU stay, 516 (21.0%) received nephrology consultations. The median time from AKI onset to nephrology consultation was 2 days (IQR, −1 to 12 days) and 282 patients (54.7%) received consultations within 48 hours of AKI onset. Among the 516 nephrology-consulted, 52 (10.1%) received consultation before AKI diagnosis (median, −1 day; IQR, −2 to −1 days); 30 (57.7%) of these 52 patients had preexisting CKD. Patients who received consultations were older and had more comorbidities (diabetes, hypertension, heart disease, and stroke) but had a lower prevalence of CKD and SIRS compared to those who did not receive a consultation (Table 1).
Outcomes
The median ICU and hospital stays were 5 days (IQR, 3–11 days) and 22 days (IQR, 13–41 days), respectively. Of the 2,416 AKI patients, 527 (21.4%) received dialysis, and 512 (20.8%) died. The median ICU and hospital stays were longer, and prescription of dialysis was more common, in patients who received nephrology consultation (Table 1). The multivariable Cox proportional hazard model revealed that nephrology consultation was associated with a significantly lower risk of in-hospital mortality (hazard ratio [HR], 0.705; 95% confidence interval [CI], 0.565–0.879). Other factors significant for in-hospital mortality were old age, SIRS, diabetes, hypertension, heart disease, cancer, higher SOFA score, and AKI stage 3 (Table 2).
Differences in the effect of nephrology consultation between surgical and medical departments
After excluding two patients without departmental information, 1,765 (71.8%) and 694 (28.2%) of 2,459 were classified as medical and surgical patients, respectively. Compared to surgical patients, medical patients had a higher incidence of diabetes, hypertension, CKD, and heart and lung diseases. At ICU admission, medical patients had a higher prevalence of SIRS and stage 3 AKI, and a greater need for dialysis, than surgical patients (Supplementary Table 2, available online).
The median lengths of ICU and hospital stays did not differ by department. There was no significant difference in the frequency of nephrology consultations between medical and surgical patients (20.1% vs. 23.2%, respectively; p = 0.09). Moreover, there was no statistically significant difference in the median time from AKI diagnosis to nephrology consultation between medical and surgical patients (2 days [–1 to 13 days] vs. 1 day [–2 to 9 days], respectively; p = 0.09).
The impact of nephrology consultation on in-hospital mortality varied between medical and surgical patients (Fig. 1). In medical patients, nephrology consultation significantly reduced the risk of in-hospital mortality (HR, 0.57; 95% CI, 0.44–0.75). However, in surgical patients, nephrology consultation was neutral for in-hospital mortality (HR, 1.09; 95% CI, 0.72–1.65) (Table 3).
Effect of nephrology consultation on patients with comorbidities and dialysis requirements
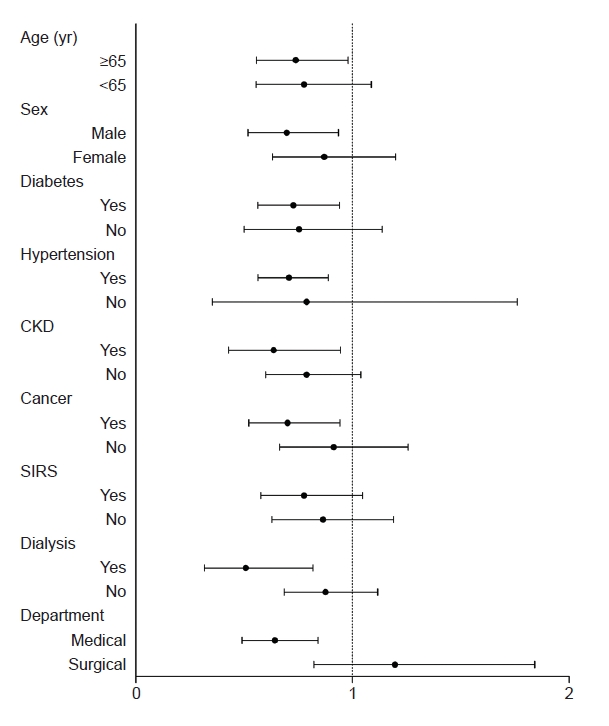
In patients with AKI admitted to ICU, the effect of nephrology consultation on in-hospital mortality varied based on baseline characteristics, comorbidities, and need for dialysis (Fig. 2). Male patients aged ≥65 years with diabetes mellitus, hypertension, cancer, or CKD, who were admitted to a medical department and undergoing dialysis, were more likely to benefit from nephrology consultation than were younger patients without comorbidities. Nephrology consultation did not affect in-hospital mortality in patients with SIRS (Fig. 2).
Outcomes by nephrology consultation time
The risks of in-hospital mortality were compared among 516 patients who received nephrology consultations during their ICU stay, and the role of early consultation was evaluated. In a multivariable analysis adjusted for age, sex, diabetes, liver cirrhosis, cancer, sepsis status, and dialysis treatment, early nephrology consultation was neutral in terms of in-hospital mortality (Supplementary Fig. 2, available online). Having diabetes (HR, 1.61; 95% CI, 1.05–2.46) or sepsis (HR, 1.61; 95% CI, 1.10–2.35) was associated with an increased risk, and treatment with dialysis (HR, 0.56; 95% CI, 0.36–0.87) was associated with a decreased risk of in-hospital mortality in this subgroup of patients.
Discussion
With recent advancements in kidney-supporting devices, increased awareness of AKI among general physicians, and easier access to RRT in the ICU, the importance of nephrology consultation is less clear and therefore requires validation. We built an AKI cohort based on EMR-extracted data for the period of 2011 to 2020, and evaluated the importance of nephrology consultation in terms of the survival of AKI patients admitted to ICUs. About 20% of the AKI patients received nephrology consultations, and their risk of in-hospital mortality was reduced by 30%. The effect of nephrology consultation varied depending on the department, comorbidities, and dialysis requirements. Old age, male sex, diabetes mellitus, hypertension, cancer, CKD, admitted to a medical department and requiring dialysis were conditions more likely to benefit from nephrology consultation. This study validated the importance of nephrology consultation in critically ill patients with AKI and provides new insights into specific conditions that can benefit from nephrology consultation.
We detected AKI retrospectively by subtracting out serum levels of creatinine; a change of ≥0.3 mg/dL within 48 hours was defined as AKI. Some of these AKI events might have been missed or unrecognized by the attending physicians at the time of ICU stay, probably explaining the relatively low rate of nephrology consultation (21.0%). In a prospective observational study in a Brazilian teaching hospital, 77 of 148 AKI patients (52.0%) consulted a nephrologist; in that study, nephrology fellows visited the ICU daily and collected all patient data. Attending physicians were thus aware that nephrologists were on alert, possibly enhancing the rate of nephrology consultation. We speculate that our findings are more reflective of the real-world scenario.
Nephrology consultations were more frequent among elderly patients with multiple comorbidities and those on dialysis, and the benefit of nephrology consultation was more pronounced in these patients. As organs interact, acute kidney illness affects other organs; subtle differences in kidney care may significantly change outcomes in patients with multiple comorbidities. We speculate that in the management of AKI, control of medical management, regulation of ultrafiltration rate [32], and timely decisions regarding the termination of dialysis [33] by nephrologists may positively affect improved survival in patients with multiple comorbidities.
The beneficial effect of nephrology consultation was more significant in medical patients than in surgical patients. This may have been because the medical patients had more comorbidities, such as diabetes mellitus, hypertension, and CKD, and a higher requirement for dialysis compared to the surgical patients. Therefore, a personalized approach based on patient characteristics and comorbidities would be more effective than simply categorizing patients as surgical or medical when determining the necessity of nephrology consultation.
Contrary to other studies [17,18,34], early nephrology consultation did not reduce in-hospital mortality, and treatment with dialysis was protective in terms of in-hospital mortality in AKI patients who received nephrology consultation. This finding may be explained by our institutional strategies. In our clinic, the decision to initiate RRT is at the attending physicians’ discretion, and once the dialysis is decided, a specialized team, that includes two skilled nurses and the first grader nephrology fellow, initiates and manages the details based on the protocol [35]. Therefore, consultation with an experienced nephrologist is still required, since the fine regulation of ultrafiltration rate or whether to terminate RRT or to transit to conventional hemodialysis requires personalized approach based on each patient’s demand-capacity balance [33]. Given our previous observations on the complex comorbidities and greater disease burden of patients who received nephrology consultations, we speculate that a timely decision to initiate dialysis by the attending physician or intensivist and sophisticated dialysis modification by a nephrologist may contribute to lower in-hospital mortality. This hypothesis requires further evaluation.
About 10% of the patients consulted a nephrologist before AKI diagnosis. We speculate that some of these were patients with oliguric AKI. Compared to creatinine, urine output is a more sensitive [36] and earlier marker of AKI [37]. Since we used serum creatinine levels to detect AKI and determined the date of AKI diagnosis based on changes therein, a delayed increase in the serum creatinine level in cases of oliguric AKI have led to an inaccurate AKI diagnosis date. Nephrology consultation prior to prescription of a nephrotoxic substance could be another explanation. In our institute, many non-nephrologist physicians consult nephrologists regarding risk management of AKI before prescribing nephrotoxic substances, such as contrast, vancomycin, colistin, or cisplatin, especially for patients with CKD. Consequently, once AKI occurred, nephrology consultation could have been recorded as preceding the AKI diagnosis date. Third, non-AKI-related consultations might have been included, because not all details of the consultations were checked due to the retrospective design of this study. This is a limitation of our study.
Another limitation of this study is that we did not check the causes of AKI or reasons for ICU admission, which might have influenced patient outcomes. Nevertheless, a notable strength of this study is the large number of AKI patients, reflecting real-world conditions.
In conclusion, nephrology consultations reduced the risk of in-hospital mortality in critically ill patients with AKI, particularly older patients with multiple comorbidities requiring dialysis. Therefore, our study emphasizes the importance of personalized nephrology consultation in the management of AKI in ICUs.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print






")









