



Introduction
Chronic kidney disease (CKD) is becoming a global health challenge [1]. Because it causes premature death and substantial healthcare costs, the increasing prevalence of CKD is a socioeconomic burden [2,3]. Diabetes mellitus (DM) is one of the most important causes of CKD in several countries [4], and the prevalence of DM in adults worldwide is expected to be 7.7% by 2030 [5]. Moreover, both DM and CKD are important risk factors for cardiovascular disease (CVD). The burden of CVD increases continuously as renal function declines [6], and individuals with both DM and CKD have an exceptionally high risk of CVD [7]. Therefore, proper DM treatment is an indispensable issue in CKD management.
Although new classes of anti-diabetes drugs have shown significant benefits in preventing CVD development [8,9], metformin is still the first-line drug for DM management [10,11]. Traditionally, metformin use has not been recommended for patients with CKD because of the risk of lactic acidosis. However, several clinical trials and observational studies have reported that the risk of fatal and nonfatal lactic acidosis did not increase with metformin use, even in patients with advanced CKD [12–14]. Accordingly, the U.S. Food and Drug Administration (FDA) of the United States expanded the criteria for metformin use. Nevertheless, prescribing metformin to advanced CKD patients, those whose estimated glomerular filtration rate (eGFR) is less than 30 mL/min/1.73 m2, remains controversial. Moreover, current clinical practice guidelines suggest diverse criteria for metformin use in patients with CKD [14], reflecting a lack of consensus about the relationship between metformin use and clinical outcomes in patients with CKD. Recent observational studies have shown inconsistent relationships between metformin use and CVD [15–17], all-cause mortality [13,18], and end-stage renal disease (ESRD) [13,19,20]. Clearly, physicians have reason to be confused about prescribing metformin to CKD patients.
Therefore, we evaluated the relationship between metformin use and the incidence of major adverse cardiac and cerebrovascular events (MACCE), all-cause mortality, and ESRD in CKD patients using data from a large Korean health screening cohort.
Methods
Study population
This retrospective observational study was conducted using cohort data from the National Health Insurance Service (NHIS) database. The NHIS data contain medical service claims, pharmacy claims, and health screening data for the whole population of the Republic of Korea. Detailed information about the NHIS database has been described previously [21]. The NHIS provides a national health screening program for adults aged ≥40 years, and approximately three-quarters of all eligible Koreans participate in those health screenings every year. Among them, we selected 267,442 individuals who participated in a national health screening between 2009 and 2015, were prescribed anti-diabetes medications, and had an eGFR of <60 mL/min/1.73 m2. From them, we excluded individuals who had type 1 diabetes (n = 4,655), had ESRD requiring dialysis or kidney transplantation (n = 583), had taken anti-diabetes medications for less than 90 days (n = 163,913), or had experienced the clinical outcomes before taking anti-diabetes medication for 90 days (n = 1,064). However, we did not exclude patients with a history of CVD, such as myocardial infarction (MI), congestive heart failure, peripheral vascular disease, or stroke. Consequently, we included 97,713 patients in this study (Fig. 1). If patients underwent multiple health screenings, they were included at the earliest health screening that satisfied the inclusion criteria. Those patients were then followed up until December 31, 2019. This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Soonchunhyang University Seoul Hospital (No. 2019-06-014) with a waiver for informed consent.
Data collection
All health screening procedures met the internal and external quality control standards of the Korean Association of External Quality Assessment Service, as judged by detailed procedures described previously [22]. Briefly, data on lifestyle habits, including cigarette smoking and alcohol consumption, were obtained using a standardized questionnaire. The laboratory measurements and anthropometric parameters were obtained by trained healthcare providers. Blood pressure was measured three times, and the average of the last two measurements was used. Blood samples were obtained after 8 hours of fasting, and eGFR was calculated using the CKD Epidemiology Collaboration equation [23]. Proteinuria was assessed by the dipstick test and was defined as ≥1+. Medication history was obtained using the prescription database of the NHIS. Metformin, sulfonylureas, thiazolidinediones, α-glucosidase inhibitors, dipeptidyl peptidase-4 inhibitors, glucagon-like peptide-1 receptor agonists, sodium-glucose cotransporter-2 inhibitors, and insulin were considered anti-diabetes medications. In addition, we collected information about the use of aspirin, statins, and renin-angiotensin system blockade (RASB). Medical histories were obtained using the diagnosis codes in the NHIS database, which are based on the Korean Classification of Disease (KCD)-7. Medical histories were confirmed when patients visited an outpatient clinic at least twice or were hospitalized at least once due to disease before their first health screening day. The Charlson comorbidity index (CCI) was calculated using medical histories [24].
Definition of metformin users
In the Republic of Korea, prescriptions for chronic diseases, including DM, are generally given for 90 days. Therefore, we defined metformin users as individuals who had metformin prescriptions for at least 90 days after the health screening day. Metformin non-users were defined as diabetes patients who had prescriptions for other anti-diabetes medications (but not metformin) for the same period. Therefore, we defined the index date of study entry as the 90th day of the anti-diabetes medication prescription after the health screening day.
Outcome assessment
The primary outcome was MACCE, a composite of nonfatal coronary heart disease (CHD) (MI and unstable angina) (KCD code I20-I23) and nonfatal stroke (ischemic and hemorrhagic stroke) (I60-I63) requiring hospitalization for more than 2 days. The secondary outcomes were incident ESRD and all-cause mortality. Incident ESRD was defined as having prescription codes for hemodialysis or peritoneal dialysis for at least 90 days or having a prescription code for renal transplantation. Mortality data were linked with data prepared by Statistics Korea that record all deaths in the Republic of Korea. As a sensitivity analysis, we used cause of death data from Statistics Korea and defined cardiovascular mortality as death caused by MACCE.
Statistical analysis
Continuous variables are expressed as means ± standard deviations, and categorical variables are presented as numbers and percentages. For comparisons between groups, Student t-test was used for continuous variables, and Pearson chi-square testing was used for categorical variables. The cumulative incidences of the outcomes were assessed using the Kaplan-Meier method. A multivariable analysis was conducted using a Cox proportional hazard regression model, and the results are expressed as hazard ratios (HRs) and 95% confidence intervals (CIs). As a sensitivity analysis, we conducted a cause-specific hazard regression analysis with mortality as a competing risk to evaluate the relationship between metformin use and MACCE or ESRD. We also used propensity score matching (PSM) analyses. The propensity scores were obtained using a logistic regression with the nearest neighbor technique, and metformin users were matched with metformin non-users in a ratio of 1:1. The logistic regression model was derived by adjusting for the following variables: age; sex; hypertension history; MI; congestive heart failure (CHF); peripheral vascular disease; stroke; cancer; use of aspirin, a statin, or RASB; body mass index (BMI); systolic blood pressure (SBP); fasting glucose; eGFR; serum total cholesterol; presence of proteinuria; smoking status with pack-years; and alcohol consumption. The PSM analyses were performed for the entire cohort and at each CKD stage. We also performed a sensitivity analysis using the subgroup with adequate adherence to anti-diabetes medication. Adequate adherence was defined as a proportion of days covered (PDC) with anti-diabetes medication greater than 80% of the entire follow-up period (PDC of metformin ≥ 80% for metformin users and PDC of other anti-diabetes medications (but not metformin) ≥ 80% for metformin non-users) [25]. Finally, we performed another PSM analysis in the subgroup whose PDC was ≥ 80%. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). A p-value of less than 0.05 was considered statistically significant.
Results
Baseline characteristics
Baseline characteristics according to metformin use are presented in Table 1. Among the 97,713 participants, 77,666 were classified as metformin users. The mean ages of the metformin users and non-users were 66.3 ± 9.5 and 66.0 ± 8.9 years, respectively. Compared with the non-users, the metformin user group was younger, more female, and had a lower history of hypertension, MI, CHF, stroke, and cancer. Thus, the CCI among the metformin users was significantly lower than that in the metformin non-users group (p < 0.001). The use of aspirin was similar between groups, but metformin users took fewer statins and RASB than non-users. In addition, metformin users had lower BMI, SBP, and serum creatinine, but they had higher fasting glucose, eGFR, total and high-density lipoprotein cholesterol, and triglyceride levels than non-users. The metformin user group had fewer smokers and individuals with proteinuria but more heavy drinkers than the non-user group.
Risk of major adverse cardiac and cerebrovascular events by metformin use status
During a mean follow-up of 5.3 years, a total of 11,434 MACCE (11.7%) occurred, for a corresponding incidence rate of 22.2 per 1,000 patient-years. The incidence rate of MACCE in metformin users was 22.5 per 1,000 patient-years, producing a significantly higher risk of MACCE than found in non-users (HR, 1.20; 95% CI, 1.14–1.26; p < 0.001) (Table 2). When comparing the components of MACCE, the risk of CHD increased marginally (HR, 1.07; 95% CI, 1.00–1.14; p = 0.05), but the risk of stroke increased significantly in metformin users (HR, 1.40; 95% CI, 1.30–1.51; p < 0.001) compared with non-users. In the cause-specific hazard regression analysis with mortality as a competing risk, metformin users still had an increased risk of MACCE (HR, 1.36; 95% CI, 1.28–1.44; p < 0.001). In the subgroups by CKD stage, the increased risk of MACCE among metformin users was observed in CKD stages 3a and 3b but attenuated in CKD stages 4 and 5 (Supplementary Table 1, available online).
Risk of all-cause mortality and end-stage renal disease by metformin use status
During the follow-up period, the incidence rates of all-cause mortality and ESRD were 24.1 and 7.6 per 1,000 patients-years, respectively. The risk of mortality during that period was significantly lower in metformin users (HR, 0.78; 95% CI, 0.74–0.81; p < 0.001) than in non-users (Table 3). The incidence of cardiovascular mortality was 3.9 and 2.8 per 1,000 patients-years in metformin non-users and users, respectively. Thus, risk of cardiovascular mortality was also significantly lower in metformin users (HR, 0.70; 95% CI, 0.62–0.79; p < 0.001) (Supplementary Table 2, available online). However, due to their increased risk MACCE, metformin users had a higher risk than non-users of experiencing the composite cardiovascular outcome (HR, 1.16; 95% CI, 1.10–1.22; p < 0.001), which was a composite of MACCE and cardiovascular mortality. In addition, the risk of ESRD was significantly lower in metformin users (HR, 0.44; 95% CI, 0.42–0.47; p < 0.001) than in non-users (Table 3). In the cause-specific hazard regression analysis with mortality as a competing risk, metformin users still had a significantly lower risk of ESRD (HR, 0.48; 95% CI, 0.44–0.52; p < 0.001) than non-users. In the subgroups of CKD stages, the lower risks of all-cause mortality and ESRD during follow-up in metformin users were consistently present in all CKD stages (Supplementary Table 3, available online).
Risk of clinical outcomes by metformin use status after propensity score matching
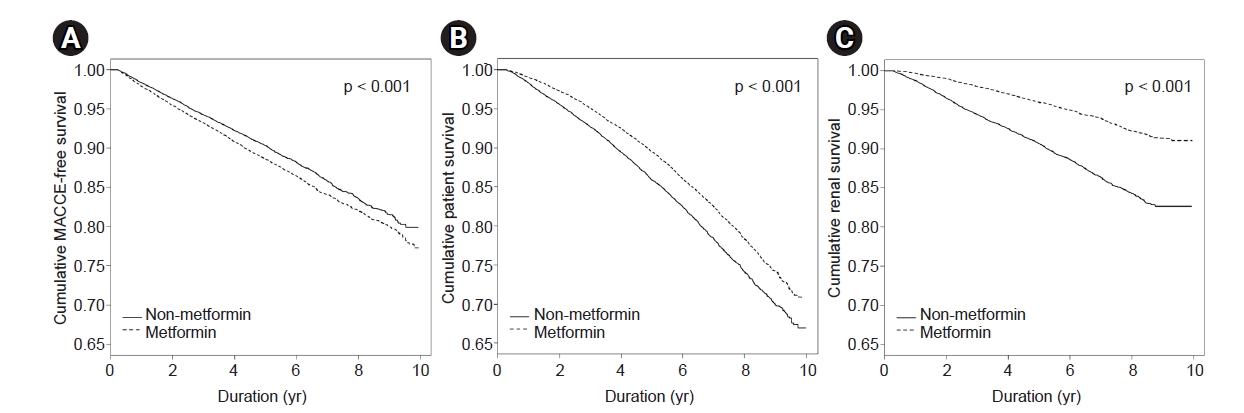
Because the patients’ characteristics differed significantly between groups, we performed PSM between metformin users and non-users in a 1:1 ratio. The baseline characteristics after PSM are presented in Supplementary Table 4 (available online). After PSM, the cumulative MACCE-free survival was significantly lower in metformin users than in non-users (p < 0.001) (Fig. 2). Meanwhile, metformin users had significantly higher cumulative survival and ESRD-free survival than non-users (p < 0.001, all). In the multivariable analysis, the HR of MACCE for metformin use was 1.15 (95% CI, 1.09–1.22) (Table 4). When we performed a PSM analysis in each CKD stage, an increased risk of MACCE was observed only in CKD stage 3a; the risk was attenuated in advanced stages. In addition, the HRs of all-cause mortality and ESRD with metformin use were 0.76 (95% CI, 0.73–0.80) and 0.45 (95% CI, 0.42–0.48), respectively, and the benefits of metformin use for delaying death and preventing ESRD were seen in all CKD stages.
Risk of clinical outcomes by metformin use status in the subgroups with adequate adherence
A further sensitivity analysis was performed in the subgroup of patients with adequate adherence to anti-diabetes medication. The metformin users in this subgroup still had a significantly increased risk of MACCE (HR, 1.66; 95% CI, 1.57–1.76; p < 0.001), and that relationship was observed in CKD stage 3, but not in stages 4 and 5 (Table 5). Furthermore, the HR for all-cause mortality during follow-up was still significantly lower for metformin users in this subgroup (HR, 0.88; 95% CI, 0.83–0.93; p < 0.001), but the survival benefit from metformin use was attenuated in patients with eGFR of <45 mL/min/1.73 m2. Meanwhile, the HR for ESRD in metformin users was 0.29 (95% CI, 0.26–0.33) and consistently lower in metformin users than in non-users in all CKD stages.
Risk of clinical outcomes by metformin use status after PSM in the subgroups with adequate adherence
Finally, we conducted PSM in the subgroup of patients with adequate adherence to anti-diabetes medication. We found that metformin use still carried a significantly increased risk of MACCE (HR, 1.65; 95% CI, 1.55–1.75; p < 0.001) (Table 6). When PSM was conducted for each CKD stage, that relationship was attenuated in the higher CKD stages, but it remained significant. Meanwhile, the survival benefit from metformin use also remained (HR, 0.89; 95% CI, 0.84–0.95; p < 0.001), but it disappeared in patients with eGFR of <45 mL/min/1.73 m2. The risk of ESRD was significantly lower in metformin users (HR, 0.30; 95% CI, 0.26–0.33; p < 0.001), and that benefit was observed in all CKD stages.
Discussion
In this study, we found that metformin use was associated with a significantly increased risk of MACCE in patients with CKD. However, metformin users had significantly lower risks of all-cause mortality and ESRD during follow-up than non-users did. These relationships were consistent in the subgroups made using a PSM analysis, adequate adherence to anti-diabetes medication, and both together. The higher risk of MACCE and lower risk of mortality during follow-up in metformin users were mitigated at advanced CKD stages; however, the benefit for ESRD was consistently shown in all CKD stages.
Although several new classes of anti-diabetes drugs have been released, metformin is still the first-line drug for DM management. In Korea, metformin is even the most commonly used anti-diabetes medication in patients with early CKD [26]. Beyond glycemic control, it has been reported that metformin has pleiotropic effects that control lipids, body weight, and blood pressure [27,28]. Nevertheless, previous studies have raised uncertainties about the effectiveness of metformin in reducing cardiovascular outcomes in the general population [29–31]. In 2016, the U.S. FDA allowed metformin use in patients with CKD stage 3, and the Korean Ministry of Food and Drug Safety followed the U.S. FDA in that ruling in 2019. However, the relationship between metformin use and cardiovascular outcomes has remained inconclusive in patients with CKD.
In a Swedish study of 51,675 patients with type 2 diabetes, treatment with metformin showed a CVD benefit when compared with insulin treatment, but not when compared with other oral hypoglycemic agents [17]. In addition, those researchers found no significant relationship between metformin use and the risk of any CVD in the subgroup of CKD stage 3 patients. Charytan et al. [15] reported that metformin users in CKD stage 3, but not those in CKD stages 4 and 5, had a lower risk of cardiovascular death than non-users. A recent study by Roumie et al. [16] reported that metformin monotherapy was associated with a lower risk of MAACE than sulfonylurea monotherapy in patients with CKD. In contrast, we found that metformin users with CKD faced a significantly increased risk of MACCE. Some patient characteristics differed between those previous studies and this study. First, the mean BMI in the studies conducted by Charytan et al. [15] and Roumie et al. [16] was greater than 30 kg/m2, which is higher than that in our study population (25.1 kg/m2). A previous study found that metformin is efficacious in lowering serum glucose regardless of BMI, but the weight reduction effect was observed only in obese patients [32]. Therefore, the cardiovascular protective effect of metformin found in previous studies might have been caused by weight reduction, which would not be expected to apply to our study population. Second, the patients in our study had a lower incidence of CHD and higher incidence of stroke than the patients in previous studies. In particular, the high risk of MACCE we found was largely caused by a high risk of stroke in metformin users, and the HR of stroke was higher than that of CHD in all our analyses. Activating the AMP-activated protein kinase (AMPK) pathway is one of the main molecular mechanisms of metformin [33]. However, AMPK activation in the brain is remarkably increased after an ischemic injury [34]. Moreover, some experimental studies have reported that metformin treatment and subsequent AMPK activation can aggravate acute cerebral infarction [35]. Importantly, at a concentration higher than the therapeutic dose, metformin can further activate the AMPK pathway [33,36]. Because metformin is eliminated by the kidney, its concentration can increase when renal function declines [37]. Therefore, a previous observational study found that metformin use was associated with an increased risk of stroke in ESRD patients on dialysis [38]. Accordingly, although we could not examine the specific doses of metformin used, high concentrations of it might have produced the high incidence of stroke and MACCE found in our study. The risk of CHD was also significantly increased in CKD stage 3 in our data. In fact, there is a lack of evidence to support increased CHD in metformin users. The high risk of CHD with metformin use might be caused by lactic acidosis [39]. However, as aforementioned, the risk of lactic acidosis with metformin use is very low, and the risk has been reported not to increase even in CKD stage 5 [12–14]. One previous study reported that metformin use could delay the endothelial recovery of a drug-eluting stent via an AMPK-dependent pathway, which could cause stent thrombosis [40]. Poor glycemic control might be another cause of the increased CHD in metformin users in our study because the baseline level of fasting glucose in metformin users was significantly higher than that in non-users. Because this study was conducted using data from a health screening cohort, we could not examine other glycemic control parameters, such as glycated hemoglobin. However, the low risk of mortality and ESRD become difficult to explain if metformin users had poor glycemic control during the follow-up period.
Despite the increased risk of MAACE, metformin users had a significantly lower risk of cardiovascular mortality than non-users in our study. Interestingly, this paradoxical result was also reported in a previous study. A post hoc analysis of a randomized controlled trial reported that patients with metformin exposure had significantly lower risks of all-cause and cardiovascular mortality during follow-up than those without exposure [41]. However, the risk of stroke did not differ between groups (HR, 0.97; 95% CI, 0.68–1.39), and the risk of MI was marginally increased in patients with metformin exposure (HR, 1.23; 95% CI, 0.92–1.65). It is difficult to find evidence to support that contradictory result. As aforementioned, although AMPK activation caused by metformin can be harmful in patients with CKD, the AMPK pathway is also a well-known underlying protective mechanism for CVD [42]. Moreover, the role of AMPK in angiogenesis is known to be contradictory. Metformin suppresses retinal angiogenesis and exerts a protective effect against retinopathy [43], and it also suppresses tumor angiogenesis [44]. On the other hand, metformin promotes angiogenesis and revascularization under hypoxic and ischemic injury [45]. Thus, AMPK activation by metformin could have different angiogenic effects in different cellular microenvironments [46], which could affect its role in the development of CVD. Moreover, the metformin users in our study were younger and had fewer comorbidities and higher eGFR than the non-users. Therefore, metformin users might have survived CVD better than non-users. In addition, because we defined our outcomes based on diagnostic codes, not medical records, our operational definitions of the outcomes might not adequately reflect real clinical events, though hospitalization with a diagnostic code is a widely used method to define outcomes in big data studies [13,16].
Metformin users had a significantly lower risk of all-cause mortality during follow-up than non-users did in our study, which is inconsistent with previous studies [15,19]. This result might reflect the lower comorbidity levels of metformin users. However, survival benefits remained when we matched comorbidities in the PSM analysis. It is noteworthy that the survival benefit of metformin use was attenuated in patients at an advanced CKD stage in our sensitivity analysis. In a study by Hung et al. [13], metformin use was associated with an increased risk of all-cause mortality during follow-up in patients with CKD stage 5. They also reported that the mortality risk increased dose-dependently with metformin use in that population. Therefore, renal function depletion and consequent metformin accumulation might not be beneficial for mortality at an advanced CKD stage. Nevertheless, that study also reported a significantly decreased risk of ESRD in CKD stage 5. In our study, the decreased risk of ESRD conferred by metformin use was observed across all CKD stages. Recent experimental studies demonstrated that metformin prevented renal fibrosis and retarded CKD progression in murine models [47,48]. Nevertheless, because metformin use also conferred an increased risk of MACCE in our study, further experimental studies are needed to reveal the effects of metformin on other organs, beyond its protective effects on the kidney.
This study has several limitations. First, because we defined metformin use as 90 days of use before the index date, we could not consider metformin use before the health screening day. Thus, the actual duration of metformin use could differ from that used in the analysis. Second, we could not consider newly added, switched, or discontinued anti-diabetes medications (other than metformin) during the follow-up period. Therefore, the effects of other anti-diabetes medications might confound our findings. Third, we could not include the dose of metformin in the analysis. Thus, dose-dependent relationships between metformin and clinical outcomes were not presented. Fourth, although we conducted PSM analyses, hidden confounding factors might still have affected the relationship between metformin use and clinical outcomes. Fifth, some health screening centers might not have used isotope dilution mass spectrometry–traceable creatinine measurements. Thus, the possibility of CKD stage misclassification exists in this study. Finally, the study population in this work was Korean, and our results might not be generalizable to other ethnic groups. Despite those limitations, our study also has several strengths. Because this was a nationwide cohort study, a large number of patients were included. In addition, the NHIS database includes claims for all medical facilities in Korea, and data from Statistics Korea include all cases of mortality. Therefore, few outcomes in the data were missing. Moreover, we conducted sensitivity analyses for subgroups with PDC of ≥80% and found consistent relationships between metformin use and clinical outcomes. Thus, our results were not confounded by medication discontinuation.
In conclusion, despite the current trend to expand metformin use in patients with CKD, we found that metformin use could be associated with an increased risk of MACCE in this population. On the other hand, metformin users had a lower risk of all-cause mortality and ESRD during follow-up than non-users did. Therefore, metformin needs to be used carefully under strict surveillance for CVD occurrence in patients with CKD.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









