Efficacy of low-dose spironolactone on top of angiotensin receptor blockade in patients with glomerulonephritis
Article information
Abstract
Background
Previous studies have shown that aldosterone antagonists have a proteinuria-lowering effect in patients with proteinuria and progressive proteinuric disease not adequately controlled by the use of angiotensin receptor blockers (ARBs). Aldosterone antagonists, in combination with ARBs, might improve proteinuria in patients with glomerulonephritis (GN).
Methods
In the present retrospective study, we evaluated the proteinuria-lowering effect and drug safety of low-dose spironolactone (12.5 mg/day) in 42 patients with GN being treated with an ARB.
Results
Proteinuria decreased from a mean total-protein-to-creatinine (TP/Cr) ratio of 592.3 ± 42.0 mg/g at baseline to 335.6 ± 43.3 mg/g after three months of treatment with spironolactone (P < 0.001). After the initial three months, the mean TP/Cr ratio increased progressively at six, nine, and 12 months; however, it was still less than the baseline value (P = 0.001, < 0.001, and < 0.001, respectively). Although serum Cr levels increased significantly at three and nine months compared with baseline (P = 0.036 and 0.026, respectively), there was no time effect of treatment (P = 0.071). Serum potassium levels tended to increase with time (P = 0.118), whereas systolic and diastolic blood pressures decreased with time (P = 0.122 and 0.044, respectively).
Conclusion
Low-dose spironolactone in combination with an ARB reduced proteinuria in patients with GN, which could represent a novel treatment option in individuals whose proteinuria is not optimally controlled by the use of ARBs alone.
Introduction
Most patients with glomerulonephritis (GN) have some risk of developing progressive renal failure. One of the most important risk factors for such progression is the degree of proteinuria. This risk might be present because proteinuria signals patients with severe glomerular injury, and proteinuria itself might be toxic to the kidney [1]. Reducing proteinuria is important because it reflects control of the primary disease and reduces glomerular hypertension (HTN) and podocyte damage. Blockade of the renin-angiotensin system (RAS) using angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) is recommended as first-line therapy to reduce proteinuria [2]. However, in many cases, ACE inhibitors and ARBs retard but do not abrogate proteinuria. Alternative or adjunctive therapies are needed in patients who have not reached their proteinuria goals despite the administration of an ACE inhibitor or ARB. Experimental animal studies have indicated that aldosterone plays a major role in the development of glomerular injury and the aggravation of proteinuria through hemodynamic and direct cellular actions. In those investigations, an aldosterone antagonist attenuated proteinuria and retarded the deterioration of renal function independently of the effects on blood pressure (BP) [3–8]. Available evidence supports the use of aldosterone antagonists in patients with proteinuria not adequately controlled by ACE inhibitors or ARBs and in patients with chronic kidney disease (CKD) [9]. Those results have also been observed in experimental animal models with GN [10–12]. The previous findings led us to hypothesize that aldosterone plays a role in the development of glomerular injury and the increased proteinuria seen in patients with GN. Thus, we conducted the current study to examine whether spironolactone, an aldosterone antagonist, in combination with an ARB ameliorates proteinuria in patients with GN already treated unsuccessfully with an ARB.
Methods
Study population
This retrospective study was conducted in accordance with the principles expressed in the Declaration of Helsinki. Clinical patient data were obtained from electronic medical records with the approval of the institutional review board of Soonchunhyang University Bucheon Hospital (IRB no. 2017-11-009). We retrospectively identified all patients who underwent a kidney biopsy at Soonchunhyang University Bucheon Hospital in Bucheon, Republic of Korea, between February 2001 and January 2017. Eligible patients fulfilled the following inclusion criteria: 1) biopsy-proven GN; 2) follow-up examinations at least three months apart with blood and urine exams for one year before and after the initiation of spironolactone; and 3) received an ARB and 12.5 mg/day of spironolactone for at least 12 months. We excluded patients with advanced CKD and those with CKD stage 4 or higher; patients who continued taking spironolactone and an ARB together after the kidney biopsy; and those who concomitantly received high-dose corticosteroids (> 15 mg/day) or another immunosuppressant agent, including cyclosporine, cyclophosphamide, or tacrolimus. Patients who were concurrently taking an ARB and an ACE inhibitor were also excluded.
Baseline characteristics at one year prior to spironolactone initiation
We obtained data on demographic characteristics and comorbidities, including history of diabetes mellitus (DM), HTN, ischemic heart disease, and hyperlipidemia. Participant body weight and height were measured and body mass index was calculated. We also investigated patient hemodynamic parameters such as systolic BP (SBP) and diastolic BP (DBP). Additionally, we obtained information about the use of anti-HTN drugs, including calcium channel blockers, beta blockers, diuretics, ACE inhibitors, and ARBs.
Pathological data
We reviewed the pathology reports from the kidney biopsies. We checked the percentage of glomeruli that showed global and segmental sclerosis to determine pathological damage. The classification of pathological severity expression differs according to the type of GN and is not used consistently, even within specific cases of GN, so all findings indicating pathological severity were reviewed. We specifically checked the pathological severity of patients with immunoglobulin A nephropathy (IgAN) according to the Lee et al [13] and Oxford classification [14].
Clinical outcomes of interest
The primary outcome in the present study was change in proteinuria over time. Secondary outcomes were adverse events, including a decrease in the estimated glomerular filtration rate (eGFR) or BP and the occurrence of an electrolyte imbalance, particularly hyperkalemia. Patients underwent regular check-ups at two- to three-month intervals. We collected laboratory data at every visit throughout the follow-up period. We obtained serum creatinine (sCr) values, eGFR values calculated from sCr via the Chronic Kidney Disease Epidemiology Collaboration equation [15], the total-protein-to-creatinine (TP/Cr) ratio, and serum sodium (Na) and potassium (K) levels at three-month intervals during the year before and after initiating spironolactone. We reviewed any administered K-lowering agents during the year after spironolactone administration.
Statistical analysis
Descriptive statistics are reported as the mean ± standard deviation for continuous variables and as the frequency with percentage for categorical variables. The mean differences from baseline at each time point were evaluated using a linear mixed model. The time effect of the variables was defined as the change of variables over time. We analyzed the statistical significance of time effects to determine whether changes in the variables after spironolactone administration were meaningful, and we also analyzed within-group differences using a linear mixed model. The following variables were adjusted: age, sex, DM, HTN, eGFR, SBP, and DBP. We used SPSS version 21 for Windows (IBM Co., Armonk, NY, USA) for the analyses, and all statistical tests were two-sided. All P values of less than 0.05 were considered to indicate statistical significance.
Results
Baseline characteristics
Among the 1,097 patients who underwent a kidney biopsy during the study period, 80 were eligible for inclusion in our analysis, but 38 of those were ultimately not considered because they met the exclusion criteria. Thus, 42 patients (24 men and 18 women; mean age, 42.2 years ± 10.0 years) were included in our analysis (Fig. 1). The baseline clinical characteristics of the study participants are presented in Table 1. HTN was the most common concomitant disease (47.6%). The included patients were taking four different types of ARBs, with most being treated with losartan (85.7%). IgAN was the most prevalent pattern of GN (71.4%), and about half of the patients were classified as above grade 4. The mean percentage of sclerosis (sum of global and segmental sclerosis) was 24.4% ± 24.3%.
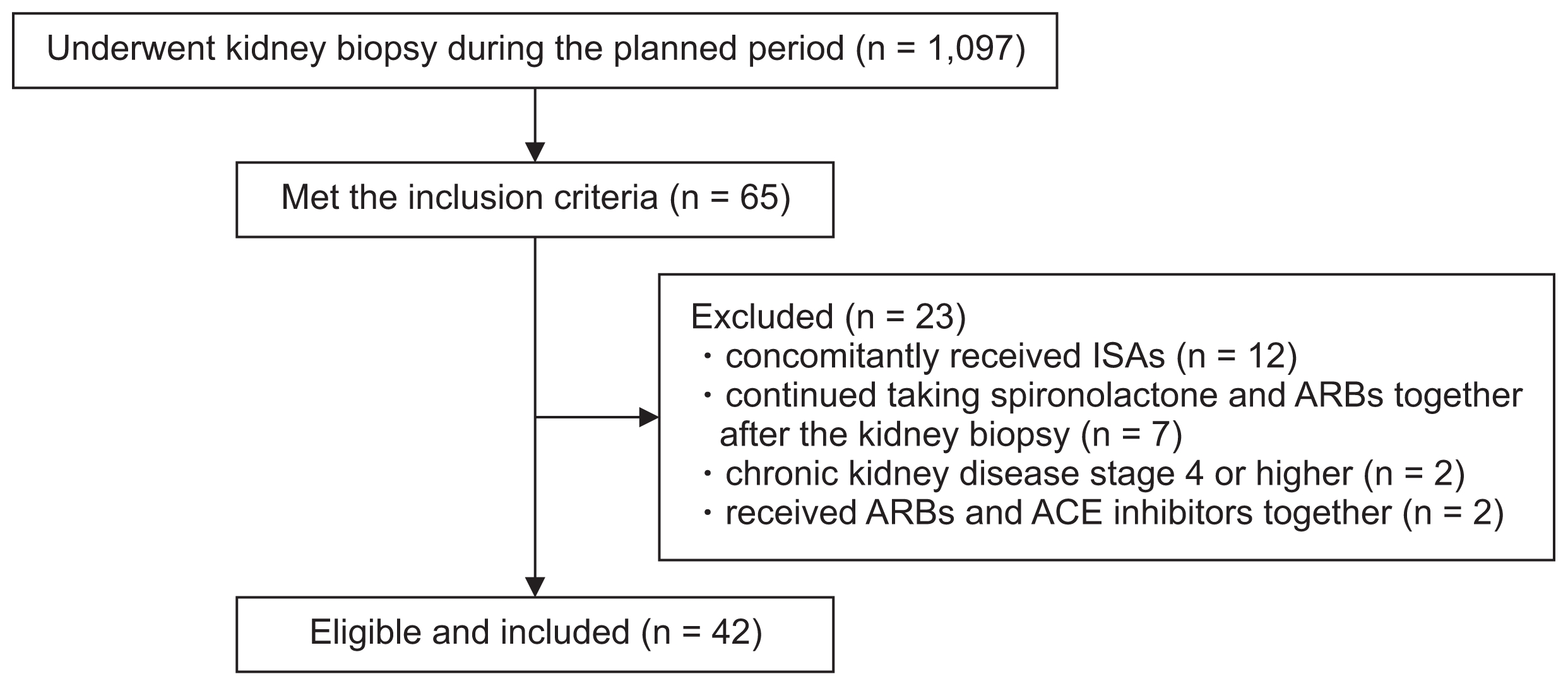
Study population
ACE, angiotensin converting enzyme; ARBs, angiotensin II receptor blockers; ISAs, immunosuppressive agents.

Baseline characteristics of all patients
Clinical outcomes of all patients
Proteinuria decreased rapidly from a mean TP/Cr ratio of 592.3 ± 42.0 mg/g immediately before spironolactone administration to 335.6 ± 42.3 mg/g after three months of spironolactone treatment and a time effect of treatment was also observed (P < 0.001). After the initial three months, the mean TP/Cr ratio increased progressively at six, nine, and 12 months; however, at all points it remained less than the baseline value (P = 0.001, < 0.001, and < 0.001, respectively) (Fig. 2). Although the sCr levels increased significantly at three and nine months compared with at baseline (P = 0.036 and 0.026, respectively), there was no time effect of treatment on the sCr levels (P = 0.071). Similarly, the eGFR decreased significantly at three months as compared with at baseline (P = 0.028), but no time effect of treatment was detected (P = 0.066) (Supplementary Table 1 and Fig. 3). Serum Na levels decreased significantly over time (P = 0.033), although there was no significant decrease in the values measured every three months compared with baseline. Serum K levels tended to increase with time (P = 0.118) (Supplementary Table 2 and Fig. 3), but no patients were given a K-lowering agent in the year after spironolactone administration. SBP and DBP decreased with time (P = 0.122 and 0.044, respectively) and showed a significant decrease at nine months compared with baseline (120.0 ± 2.4 to 110.9 ± 2.4, P = 0.021 and 74.5 ± 1.4 to 69.3 ± 1.1, P = 0.044, respectively) (Supplementary Table 2 and Fig. 4).

Changes in the total-protein-to-creatinine (TP/Cr) ratio in all patients from 12 months before to 12 months after the onset of spironolactone treatment
*P < 0.05 vs. baseline levels; †time-effect was tested by linear mixed model, and the following variables were adjusted: age, sex, diabetes, hypertension, estimated glomerular filtration rate, and systolic and diastolic pressure.
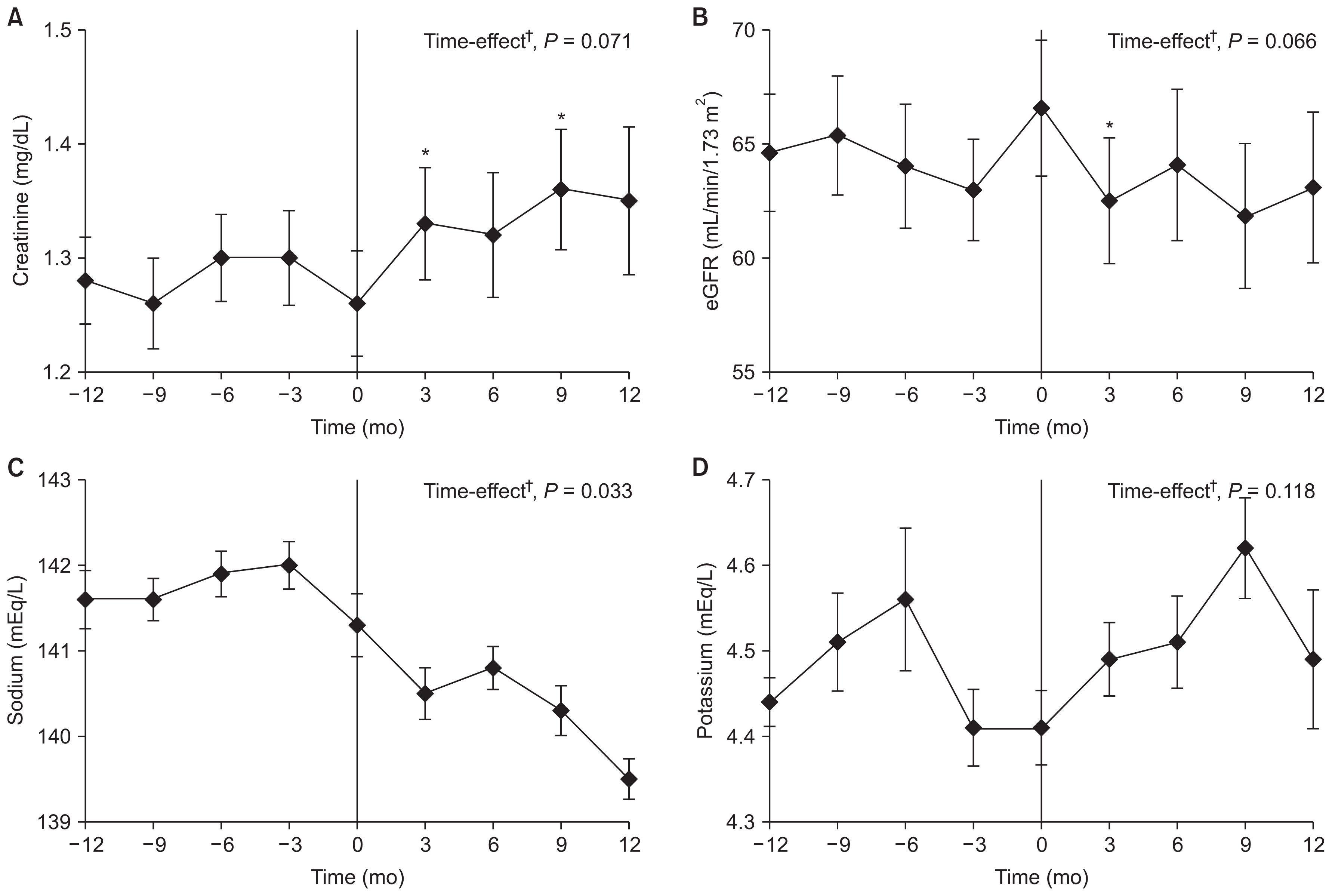
Changes in serum creatinine (A), estimated glomerular filtration rate (eGFR) (B), sodium (C), and potassium (D) levels in all patients from 12 months before to 12 months after the onset of spironolactone treatment
*P < 0.05 vs. baseline levels; †time-effect was tested by linear mixed model, and the following variables were adjusted: age, sex, and systolic and diastolic pressure.
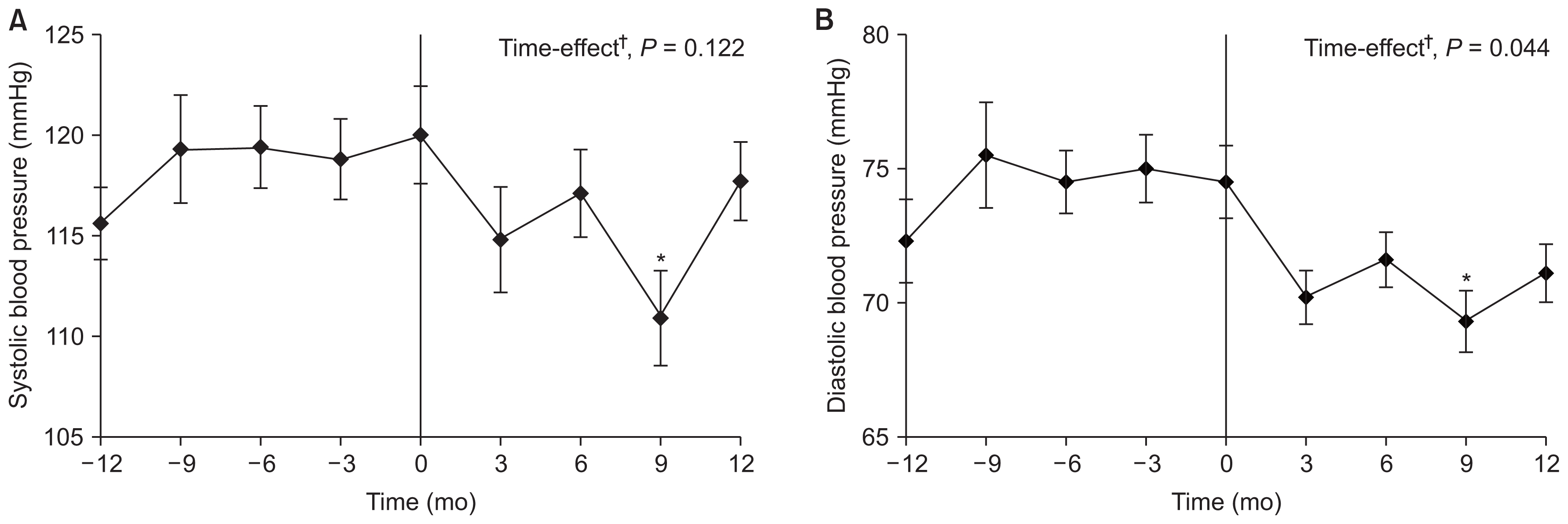
Changes in systolic (A) and diastolic (B) blood pressure in all patients from 12 months before to 12 months after the onset of spironolactone treatment
*P < 0.05 vs. baseline levels; †time-effect was tested by linear mixed model, and the following variables were adjusted: age, sex, diabetes, hypertension, and estimated glomerular filtration rate.
Clinical outcomes according to the pathological findings
A significant decrease was observed in the TP/Cr ratio over time in the low- and high-grade IgAN groups (P = 0.030 and 0.001, respectively). However, no significant difference between the two groups was observed in the time effect of treatment (P = 0.220). The TP/Cr ratio decreased significantly at all time points compared with baseline in the high-grade group; however, it decreased only at 12 months in the low-grade group (Supplementary Table 3 and Fig. 5). No significant difference between the two groups was observed in the time effect of treatment on sCr level, eGFR, serum Na and K levels, SBP, or DBP (P = 0.339, 0.658, 0.896, 0.517, 0.213, and 0.700, respectively) (Supplementary Table 4, 5). A time effect of treatment was observed in the TP/Cr ratio regardless of Oxford classification, and there was no significant difference in the time-group effect according to the MEST-C score of the Oxford classification (P = 0.707, 0.828, 0.559, 0.728, and 0.916 for M-, E-, S-, T-, and C-scores, respectively). Futher details on Supplementary materials are presented online (available at https://doi.org/10.23876/j.krcp.2018.37.3.257).

Changes in the total-protein-to-creatinine (TP/Cr) ratio according to the severity of pathologic findings from 12 months before to 12 months after the onset of spironolactone treatment
*P < 0.05 vs. baseline levels; †comparing the time-effects of two groups; and ‡the time-effect of each group was tested by linear mixed model, and the following variables were adjusted: age, sex, diabetes, hypertension, estimated glomerular filtration rate, and systolic and diastolic pressure.
IgAN, immunoglobulin A nephropathy.
Discussion
We designed the current study to evaluate the efficacy and safety of using an aldosterone antagonist to reduce proteinuria in patients with GN. To our knowledge, no previous studies have confirmed the proteinuria-lowering effect of aldosterone antagonists in patients with GN, although there is strong a priori evidence [9,16,17] for it through the extrapolation of results with DM nephropathy and CKD patients. Those previous studies showed that a spironolactone dose of 25 mg/day reduces proteinuria. In our center, a patient with GN who shows a sudden increase in proteinuria is rechecked for the amount of proteinuria one month later. Subsequently, we administer 12.5 mg/day of spironolactone to those patients whose proteinuria continues to increase but remains too low to require an immunosuppressant. We evaluated whether proteinuria could be reduced by using only half the dose of the previous study dose under the hypothesis that the lower dose could reduce the incidence of decreased kidney function, hyperkalemia, and hypotension while maintaining the effect of proteinuria reduction. In the current study, the proteinuria-lowering effect was observed three months after the start of spironolactone administration and was maintained for one year.
These results correspond with an earlier study that reported that proteinuria was significantly reduced by the use of aldosterone antagonists in patients with DM nephropathy and CKD. Notably, the time effect of treatment was not significant with respect to sCr levels or eGFR, which we used to evaluate kidney function. However, those variables deteriorated significantly from the baseline values at an early time point, suggesting that attention should be paid to worsening kidney function at the beginning of spironolactone administration in patients with GN. A significant decrease in serum Na levels was observed over time, but the values remained clinically acceptable. In terms of drug safety, K levels tended to increase, but none of the patients needed a K-lowering agent. Unlike in previous studies [9,17], the patients in our study experienced significantly decreased BP over time, particularly nine months after the start of spironolactone treatment. However, no sharp decrease in mean BP was observed during the same period, and BP increased again by 12 months. Because a BP-lowering effect was seen after nine months, this effect might have been missed by the previous studies, which included six months or less of follow-up time. Therefore, close BP monitoring is required in all patients receiving spironolactone treatment, with particular attention paid to those with a low BP before spironolactone administration. The BP-lowering effect could actually be helpful for patients with HTN that is not well-controlled. Because the current study included only patients with GN, the effect of spironolactone was analyzed according to pathological findings. We analyzed whether the proteinuria-lowering effect of spironolactone differed according to the Lee and Oxford classifications of IgAN patients. A time effect of treatment was observed on the TP/Cr ratio regardless of pathological severity; however, no difference was observed in terms of the time–group effect according to both the grade and MEST-C scores of the Lee and Oxford classification, respectively. This finding suggests that spironolactone had a proteinuria-lowering effect regardless of pathological severity in patients with IgAN. No significant decrease in BP was observed when we analyzed our results according to the pathological findings.
A RAS blockade ameliorates the deterioration in glomerular structure and function and interferes with the cellular and glomerular hypertrophy that could lead to glomerular sclerosis [18–20]. In the past few decades, experiments in rat models [21,22] and human studies [23–26] have suggested that blocking the RAS with an ACE inhibitor or ARB slows the progression of renal disease. A RAS blockade has thus become a leading therapeutic strategy for the treatment of progressive renal disease. However, in some patients, renal disease continues to progress despite treatment with an ACE inhibitor or ARB. Several studies have shown that a RAS blockade does not uniformly suppress the RAS. After several weeks of using of an ACE inhibitor or ARB, plasma aldosterone return to pretreatment levels in 30% to 40% of patients [27]. One year after initiating ARB treatment, an increase in the serum aldosterone level > 10% over baseline was observed in 28% of patients [28]. Plasma aldosterone levels tend to increase over time during treatment with an ACE inhibitor or ARB (i.e., aldosterone breakthrough phenomenon) [29–31]. Previous studies suggested that ACE inhibitors or ARBs are insufficient to suppress aldosterone synthesis and that an aldosterone blockade together with a RAS blockade would be effective. Thus, clinical interest in the renoprotective effects of an aldosterone blockade has increased enormously over the years.
Glomerular injuries, including glomerulosclerosis and interstitial fibrosis, tend to progress over time even when the primary insult to the kidneys has been ended or corrected. Experimental animal studies indicate that aldosterone plays a major role in the development of glomerular injury, possibly through its nongenomic effects, including inflammation, fibrosis, and oxidant injury [32]. An experimental rat model documented that aldosterone antagonists retard the development of glomerulosclerosis and induce the regression of existing glomerulosclerosis [33]. Previous studies showed that an aldosterone blockade further decreased proteinuria in DM patients already being treated with an ACE inhibitor or ARB [16,34]. This effect was also seen in a study of patients with CKD [9,17]. Thus, an aldosterone blockade might have an additive renoprotective effects in humans. Our current study is meaningful because it shows that those effects are also present in patients with GN.
However, the current study also has several limitations, such as a small sample size and a retrospective design. Although this work involved a longer study period than previous investigations, its duration was still insufficient to assess the long-term effects of spironolactone on proteinuria and kidney function. Second, several variables were inaccurately measured, and important variables could not be obtained. We were unable to perform 24-hour ambulatory BP monitoring or daily home BP measurements, making it difficult to measure the exact average BP. In our center, we measure BP at least twice at each clinical visit and record the average of those measurements. We collected information about BP measured in this way through the patient medical records. However, that method is inadequate compared with 24-hour ambulatory BP monitoring or daily home BP measurements. Additionally, we evaluated the degree of proteinuria through the TP/Cr ratio. Although a close correlation between the TP/Cr ratio and 24-hour protein excretion has been documented in patients with primary glomerulopathies [35], 24-hour urine collection remains the gold standard method for determining protein excretion. Therefore, the amount of proteinuria measured by the TP/Cr ratio is likely to be somewhat different from the actual value. In terms of pathological findings, variability between patients in the number of glomeruli obtained meant that the percentage of global and segmental sclerosis could not be exactly determined. The major limitation of this study was that we could not obtain information about baseline or changes in serum aldosterone levels, and thus we could prove objectively whether spironolactone actually suppressed aldosterone. Therefore, we cannot explain the precise mechanism by which spironolactone reduces proteinuria but can only make assumptions about the mechanism involved based on previous research. Third, we did not include a nontreatment reference group that received an ARB alone, which limited the extent of our analysis. At the time of study design, we decided to consider patients treated with only an ARB as a control group (ARB-only group) for comparison with patients receiving spironolactone (spironolactone group). However, it was difficult to find suitable patients treated with only ARB who showed a sudden increase in proteinuria after showing stable maintenance for one year without immunosuppressive treatment, as in the spironolactone group. There was also concern that selection bias might occur when determining a specific period (two years) for comparison with the spironolactone group. Instead of comparing the data with a reference group, therefore, we compared changes in laboratory data taken one year before and after the onset of spironolactone administration. In that way, we determined that there was no significant difference in sCr level or changes in eGFR after spironolactone administration.
This study evaluated the use of low-dose spironolactone, an aldosterone antagonist, in combination with an ARB to improve proteinuria in patients with GN already treated with an ARB. We suggest that low-dose spironolactone in combination with an ARB could be a suitable therapeutic option for patients with GN whose proteinuria is not optimally controlled by an ARB. Despite the low dose, spironolactone administration can cause side effects such as worsening of kidney function and lowering of BP. Therefore, even with a low dose, spironolactone should be prescribed with caution. Randomized controlled studies with long-term follow-up are needed to fully assess the efficacy and safety of low-dose spironolactone in patients with GN.
Supplementary Data
Acknowledgments
This work was supported by the Soonchunhyang University Research Fund.
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.