


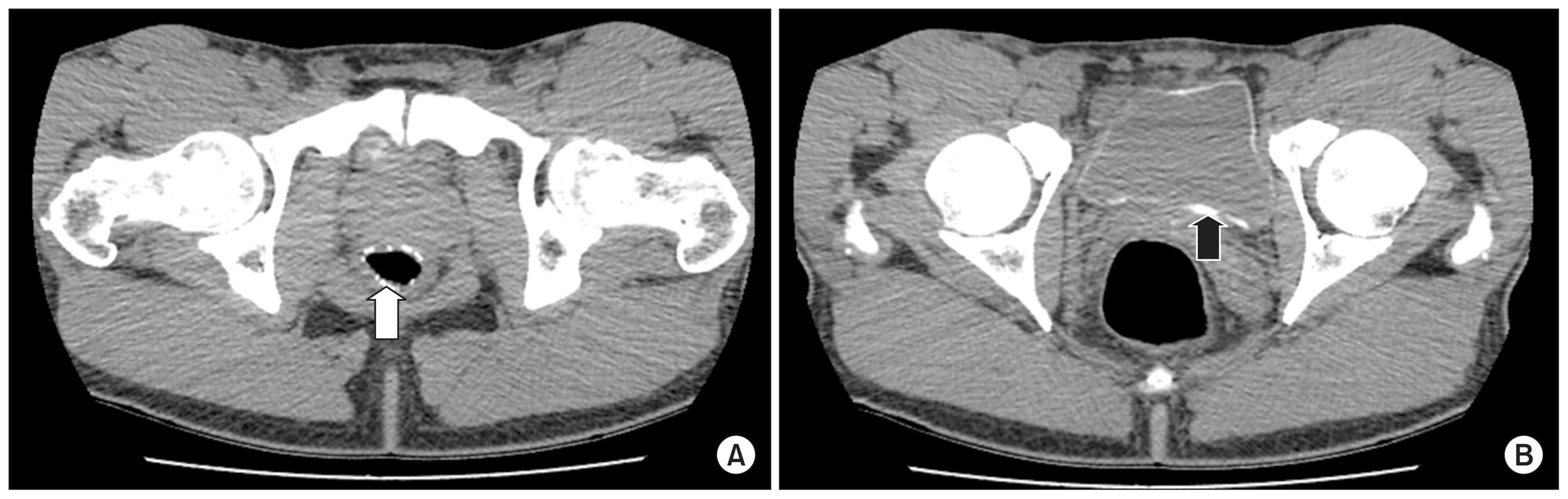
A 28-year-old Ghanaian man presented with a 1-month history of lower abdominal pain. The patient reported experiencing similar episodes several times over the past two years. He had no medical or surgical history. The physical examination was unremarkable. Blood tests, including eosinophilia (1.4%), were within normal limits. Urinalysis presented no eosinophiluria, hematuria, or pyuria. Urine cultures were sterile. Computed tomography (CT) scan of the abdomen and pelvis without administration of intravenous contrast medium demonstrated mural calcification of the left ureter (Fig. 1, white arrow) and circumferential curvilinear calcification of the urinary bladder (Fig. 1 and 2, black arrows). There was also calcification of the wall of the rectosigmoid bowel (Fig. 2, white arrow). No parasitic eggs were identified in urine cytology. Serum schistosoma antibody was positive for Schistosoma mansoni and Schistosoma haematobium.
Schistosomiasis is an endemic parasitic infection caused by trematodes of the genus Schistosoma. These parasites are endemic to Africa, India, Central and South America, and the Middle East. Korea is a non-endemic area because there is no intermediate host, Biomphalaria. However, schistosmiasis is expected to become more common as more foreigners enter Korea.
The diagnosis of schistosomiasis requires detection of infection by direct assays including demonstration of eggs in the stool or urine via microscopy; demonstration of schistosome antigen or DNA in the blood, urine, and/or stool; and indirect assays including demonstration of antibody in blood via serology. Serologic tests are a useful diagnostic tool in the absence of egg detection via microscopy. In our case, we tried to identify eggs in urine but found no parasitic eggs in urine cytology. The assays available for demonstration of antibody include enzyme-linked immunosorbent assay (ELISA), radioimmunoassay, indirect hemagglutination, western blot, and complement fixation. We identified the antibody against S. mansoni and S. haematobium in patient serum by ELISA. Because the patient had already been in Korea for 3 years, identifying the direct source of the parasite infection might be impossible. Calcifications, usually first identified along the bladder base in a fine linear pattern, that extend to include the entire bladder circumference are characteristic CT findings of chronic genitourinary schistosomiasis, in which the larvae of the schistosoma parasite are deposited on the walls of the organs and become calcified. In areas where S. haematobium is endemic, schistosomiasis is the most common cause of bladder wall calcification, with the degree of calcification proportional to the number of dead eggs trapped in the bladder submucosa. In Korea, an area with endemic tuberculosis, this disease may also cause calcification of the bladder wall and should be considered in the differential diagnosis.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









