



Introduction
Ambient air pollution is comprised of a variety of factors. Since 1990, both morbidity and mortality have been continuously increasing due to air pollution. In 2015, the number of deaths caused by exposure to particulate matter with aerodynamic diameter less than 2.5 ╬╝m (PM2.5) was estimated at 4.2 million, and it was the fifth-ranking mortality risk factor [1]. Interest in premature death due to PM2.5, ozone (O3), and carbon monoxide (CO) exposure has increased remarkably. PM2.5 and O3 exposure has been reported to be the cause of preventable deaths in Southeast Asia, and research predicts that this impact will more than double by 2050 [2].
A linear relationship between PM2.5 concentration and the risk of incident chronic kidney disease (CKD) and progression to end-stage renal disease (ESRD) has been observed [3]. Recent studies have drawn attention to the increased risk of chronic disease caused by exposure to atmospheric CO. A time-series study conducted on the elderly population older than 65 years in the United States reported that short-term exposure to CO increased the risk of emergency hospitalization for cardiovascular disease [4]. A case-crossover study conducted on individuals belonging to similar age groups across seven Australian cities showed similar results [5]. An increase of 10 ppm in CO level elevated the relative risk of heart failure by 1.37-fold, while a 1 mg/m3 increase in CO level was associated with increased all-cause mortality and cardiovascular mortality [6ŌĆō8]. In a large-scale cohort study conducted in the United States, higher CO concentration was associated with decreased glomerular filtration rate and increased risk of CKD and ESRD progression, similar to that observed in other studies [9].
However, few studies have examined the correlation between air pollution and prognosis of the dialysis-dependent population. It is difficult to ascertain the impact of air pollution on health. Here, we conducted a case-control design study to overcome the limitations of time-series studies and confirm the transient and acute effects of causative factors in epidemiological studies. We analyzed the association between atmospheric CO concentration and mortality risk in patients undergoing hemodialysis.
Methods
Kidney Dialysis Registry of the Korean Society of Nephrology and study population
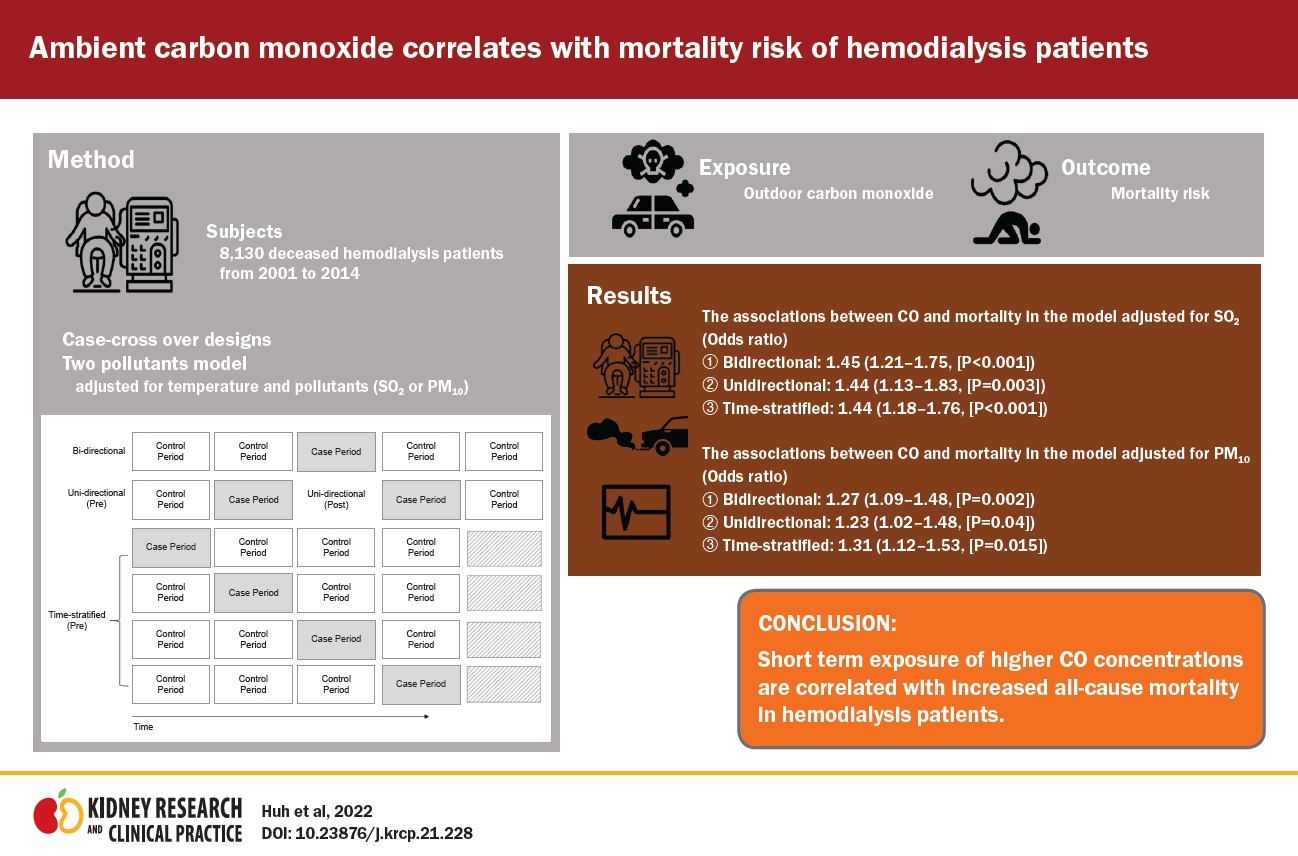
We used the Kidney Dialysis Registry database of the Korean Society of Nephrology (KSN), in which two-thirds of all dialysis patients in South Korea are registered. Included subjects were deceased patients who underwent maintenance hemodialysis and whose address information could be confirmed. From 2001 to 2014, we enrolled 8,130 deceased hemodialysis patients from the KSN [10]. The KSN registry has been used in various studies of dialysis patients in South Korea. The registry includes basic demographic information such as age and sex and information on underlying disease including hypertension and diabetes mellitus, causative diseases of ESRD, laboratory findings, dialysis adequacy, and currently applied dialysis modality [11].
Ethics consideration
Ethical approval was obtained from the Institutional Review Board of Seoul National University Hospital (No. H-2004-048-1116). All methods were performed in accordance with the relevant guidelines and regulations of the Declaration of Helsinki and received full internal approval.
Variable ambient air pollution data, including CO concentration
Information on air pollution and climate (temperature), including CO concentration, during the study period (2001ŌĆō2014) was collected from 89 monitoring sites located within seven cities and aggregated. Data included concentrations of CO, nitrogen dioxide (NO2), sulfur dioxide (SO2), O3, and particulate matter less than 10 ╬╝m in diameter (PM10). All data except O3 concentration were described as average values over 24 hours. The maximum value was reported for O3 level. All data were obtained from the Korean National Institute of Environmental Research. Collected data about weather and air pollution were used in the same manner as in the study population [12].
Study design
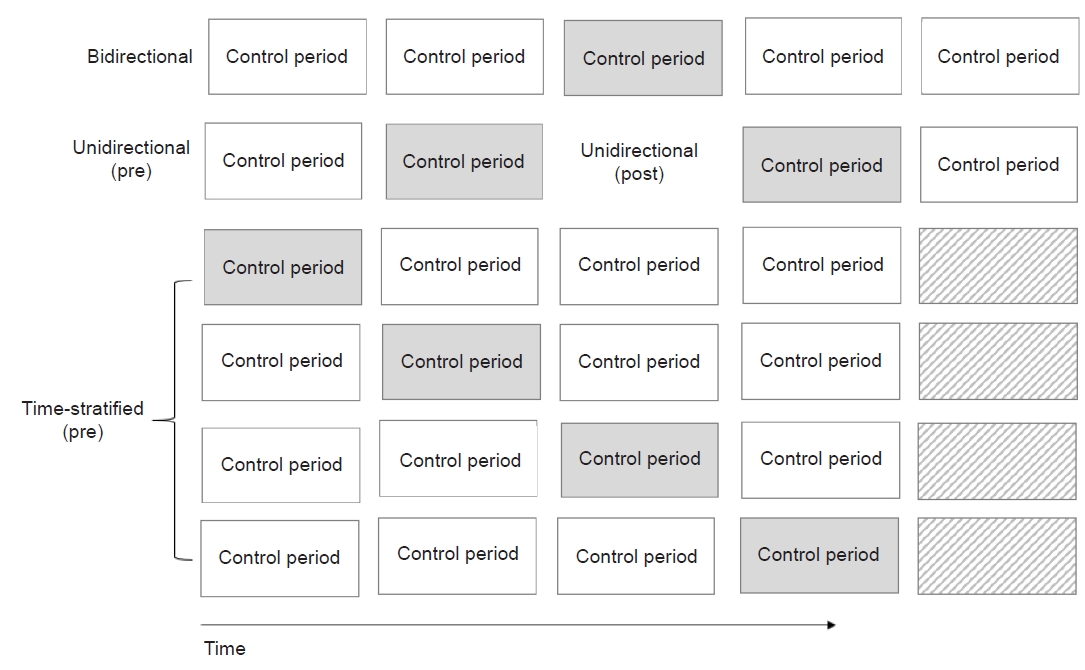
We applied case-crossover designs with different control period selections as shown in Fig. 1. Three models of case-crossover design that included bidirectional, unidirectional, and time-stratified designs were used to estimate the association between short-term exposure to CO and mortality risk in hemodialysis-dependent patients by comparing the respective control selections. This statistical method evaluates the risk of exposure factors by comparing exposure levels in the period when the event occurred (case period) with that when it did not occur (control period) to reduce the influence of uncontrolled confounding factors between subjects. As the case and control subjects are identical, the effects of age, sex, genetic predisposition, socioeconomic status, and seasonality are controlled [13ŌĆō15]. Subject death was defined as the case period.
The first design was the bidirectional method, which is a two-to-one matched case-control study that sampled control periods as the exposure 7 days before and 7 days after the date of the event. The second design was the unidirectional method, which was selected as the exposure 7 days before (pre-) or 7 days after (post-) the event day. The third design was a time-stratified design matched on the day of the week, which was selected with a 3-day exclusion period around the event day in the same month. Pollutant concentrations on the day of the event (lag 0) up to the previous 10 days (lag 10) were used to determine the exposure pattern with the strongest association. Daily CO concentrations during the case and control periods were compared between the three case-crossover designs. We mainly used a two-pollutant model, adjusted for temperature as a climate factor and adjusted for SO2, NO2, O3, and PM10 as air pollution variables other than CO.
Statistical analyses
We used conditional logistic regression analysis via the Cox proportional hazard function for analysis. Data are expressed as the odds ratio (OR) and 95% confidence interval (95% CI). The conditional logistic model can be simplified by the following formula after matching for time-invariant individual risk factors:
In this model, ╬▓1, ╬▓2, and ╬▓3 represent the vectors whose components denote the log odds of mortality associated with CO, temperature, and other air pollutants, respectively, as confounders. Using the formula above, Yij ŽĄ {0,1} represents the case status (case = 1, control = 0) of the jth observation of the ith strata, where ╬▒i is the constant term of ith strata. The ambient temperature, which is a stationary confounding factor, and air pollutants (PM10, NO2, SO2, and O3) were incorporated into each model. The CO effect was estimated based on its single lag daily mean, and we examined the association with single-day lags (from lag 1 to lag 10) and multiday lags (moving average lag 0ŌĆō1 to lag 0ŌĆō10).
Results
Baseline characteristics of the deceased
We identified death events of 8,130 hemodialysis patients between 2001 and 2014 in seven metropolitan cities in South Korea. The average age at death was 66.21 ┬▒ 12.13 years, and the proportion of males was 59.1%. The prevalence of diabetes and hypertension was 55.6% and 35.5%, respectively. The most common causative diseases of ESRD were diabetes (55.8%) and hypertension (14.4%), with unknown causative disease in 13.1% of cases. Excluding ŌĆ£others,ŌĆØ cardiovascular disease (35.5%) was the most common cause of death, followed by infection (20.3%) (Table 1). The numbers of deaths during the study period according to the city and information on climate and air pollution are presented in Table 2. In Seoul, Daegu, and Daejeon, CO concentrations of 1.002, 1.025, and 1.096 ppm, respectively, were found to be above the 90th percentile.
Effect of CO exposure on mortality of hemodialysis patients
In the single-pollutant model, we found a significant association between CO exposure and all-cause mortality (bidirectional: OR, 1.20 [95% CI, 1.04ŌĆō1.39]; unidirectional: OR, 1.45 [95% CI, 0.95ŌĆō1.38]; and time-stratified: OR, 1.19 [95% CI, 1.02ŌĆō1.38]). In the two-pollutant model adjusted for temperature and other air pollutants including SO2 and PM10, there was a significant association between CO exposure and all-cause mortality (Table 3). Associations were observed in the three case-crossover designs (bidirectional: OR, 1.45 [95% CI, 1.21ŌĆō1.75], p < 0.001; unidirectional: OR, 1.44 [95% CI, 1.13ŌĆō1.83], p = 0.003; and time-stratified: OR, 1.44 [95% CI, 1.18ŌĆō1.76], p < 0.001) in the model adjusted for SO2. Moreover, patients with comorbidities (diabetes) and older age (>75 years) had higher mortality after CO exposure in the model adjusted for SO2. Patients with diabetes (bidirectional: OR, 1.42 [95% CI, 1.11ŌĆō1.81], p = 0.005; unidirectional: OR, 1.53 [95% CI, 1.11ŌĆō2.12], p = 0.01; and time-stratified: OR, 1.52 [95% CI, 1.17ŌĆō1.97], p = 0.002) or those aged >75 years (bidirectional: OR, 1.45 [95% CI, 1.14ŌĆō1.84], p = 0.002 and time-stratified: OR, 1.44 [95% CI, 1.12ŌĆō1.86], p = 0.005) had higher risks of mortality than patients without diabetes or individuals aged <75 years (Table 4). Control time sampling had significant differences, with bidirectional sampling of control time having the smallest p-value compared with the other two designs. The effect of CO on all-cause mortality in hemodialysis patients showed similar results in the two-pollutant model adjusted for PM10. In addition, patients with diabetes had higher risk of mortality than patients without diabetes in the two-pollutant model adjusted for PM10. Furthermore, in the three-pollutant model adjusted for SO2 and PM10, we observed a significant effect of CO in the case-crossover designs (bidirectional: OR, 1.29 [95% CI, 1.10ŌĆō1.50]; unidirectional: OR, 1.24 [95% CI, 1.01ŌĆō1.51]; and time-stratified: OR, 1.25 [95% CI, 1.06ŌĆō1.47]). We found a similar association of CO with all-cause mortality in the other two-pollutant models adjusted for NO2 and O3, respectively (Supplementary Table 1, available online).
We performed subgroup analysis to identify mortality risk according to factors related to hemodialysis, and patients with anemia (hemoglobin of <10 mg/dL) had increased risk of mortality (bidirectional: OR, 1.57 [95% CI, 1.12ŌĆō2.22] and time-stratified: OR 1.49 [95% CI, 1.03ŌĆō2.15]). However, there was no increased risk of mortality according to blood pressure or dialysis adequacy (Supplementary Table 2, available online). For sensitivity analysis, we performed further analysis according to cause of death. Similar to the risk of all-cause mortality, increased risks of cardiovascular and infection-related mortalities were observed in the two-pollutant model adjusted for PM10 (Supplementary Table 3, available online).
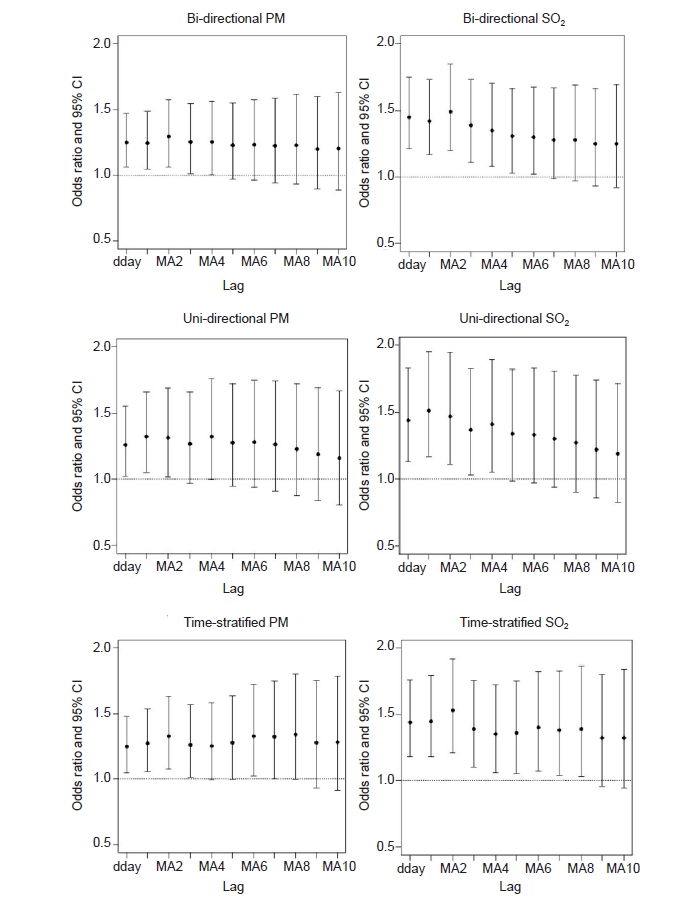
Moving average
The moving average from lag 10 to the event day (death) is shown in Fig. 2. The moving average in the three case-crossover designs was compared. In the case-crossover design adjusted for daily SO2 concentration, there was a significant association between CO exposure and mortality observed 6 days (bidirectional), 4 days (time-stratified), and 8 days (unidirectional) before the event (Supplementary Table 4, available online). We observed a short lag effect of CO exposure throughout the moving average.
Discussion
Air pollution is a global economic burden as it is known to directly increase morbidity and mortality in humans in addition to impact the climate and environment. The effects of air pollution on cardiovascular and respiratory disease, including stroke, have been studied [16ŌĆō18]. Among the air pollutants, CO concentration varies according to region and season, although it is known to be higher in urban areas [19]. A number of studies have been conducted on the effects of short-term exposure to elevated CO levels in patients with chronic diseases [20]. These effects have also been studied in patients with CKD; however, few studies on the effects of CO exposure on dialysis patients have been conducted.
To examine the association between short-term CO exposure and all-cause mortality in hemodialysis patients, we used three model case-crossover designs that can significantly reduce the impact of confounding factors. Moreover, we compared the results of various selection schemes in the case-crossover design and found no difference in the association between CO exposure and death in hemodialysis patients. Among patients undergoing hemodialysis, mortality risk was higher in those with diabetes or those aged >75 years. Our study showed that short-term exposure to elevated ambient CO level can increase the risk of death in patients with ESRD, with older adults and those with concomitant diabetes being more susceptible. The moving average is commonly used with time-series data to smoothen short-term fluctuations. The results suggest that CO has a mediating effect on the death of hemodialysis patients. A study conducted in South Korea using case-crossover time-stratified analysis demonstrated a correlation between CO exposure and cardiovascular and all-cause mortality in those with manual occupations or aged 65 to 74 years [21]. A 2-year prospective observational study of 256 elderly hemodialysis patients in Taipei showed that the risk of stroke and cardiovascular disease was higher in patients living in areas with severe air pollution or in those with lower serum albumin level. Researchers have attributed this to protein-energy wasting syndrome [22]. In Australia, an analysis using a case-crossover model involving 1,158,891 patients found that the elderly (aged >65 years) had an increased risk of hospitalization for all types of cardiovascular disease [5]. These findings are consistent with our results, which showed that elderly patients are vulnerable to outcomes caused by short-term exposure to elevated CO concentration. Although the type of cardiovascular disease could not be identified, the main causes of death in our study subjects were cardiovascular disease and infection. Consistent with previous studies on the risks of cardiovascular disease, our study demonstrates the potential for increased risk of cardiovascular disease in hemodialysis patients due to CO exposure.
There are many hypotheses about the mechanism by which ambient CO affects the organs in the human body. It has been reported that exposure to CO concentration much higher than ambient increases carboxyhemoglobin level, resulting in myocardial ischemia [23]. With regard to CO poisoning, a correlation between reduction in ejection fraction and degree of CO exposure has been observed [24]. Some studies have also found an increased risk of long-term arrhythmia after CO poisoning [25]. The first mechanism to be considered is that the binding capacity of CO to hemoglobin is more than 200 times higher than that of oxygen [26]. There is a possibility that organ ischemia can occur due to elevated carboxyhemoglobin level in a vulnerable group with cardiovascular risk. Although the study was conducted on peritoneal dialysis patients, researchers suggested a relationship between CO exposure and secondary hyperparathyroidism [27]. Considering studies that show a correlation between CO exposure and uremic pruritus [28], it is highly likely that CO exposure has an additional effect on ESRD patients.
Although most studies on air pollution and risk of infection have focused on the relationship between fine particulate matter and respiratory infection, air pollution has also been shown to be associated with peritoneal-related infections and pneumonia [29]. Some investigators have proposed mechanisms for adverse responses, including cardiac dysfunction, CO-dependent reactive oxygen signaling events, and interference with homeostasis [30]. A recent hypothesis is that exposure to air pollutants through the respiratory tract stimulates the lung autonomic nervous system (ANS), leading to oxidative stress that causes ANS imbalance and systemic vasculature damage, including the heart [31]. However, contrary to these theories, there are also claims that CO has a protective effect. Researchers in Hong Kong found that exposure to CO reduces the risk of hospitalization for respiratory infections [32]. In addition, animal studies have reported a protective effect of CO exposure against acute kidney injury and sepsis [33,34].
The method used in our study has the advantage of low risk of bias as the influence of confounding factors is reduced. In addition, the results were compared in three models. However, our study has some limitations. We accounted for known confounders but could not exclude the possibility of residual confounders (either those unmeasured or unknown). Our database did not contain information on time spent in traffic or outdoors, which can result in misclassification of exposure.
In conclusion, our findings are consistent with the notion that limited exposure to CO is associated with various adverse outcomes and high mortality in patients with ESRD dependent on hemodialysis. These results suggest that avoidance of CO exposure could be correlated with survival benefit among hemodialysis patients and provide an important clue to improve patient survival.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









