Novel biomarkers for diabetic kidney disease
Article information

Abstract
Although diabetic kidney disease (DKD) remains one of the leading causes of reduced lifespan in patients with diabetes mellitus; its prevalence has failed to decline over the past 30 years. To identify those at high risk of developing DKD and disease progression at an early stage, extensive research has been ongoing in the search for prognostic and surrogate endpoint biomarkers for DKD. Although biomarkers are not used routinely in clinical practice or prospective clinical trials, many biomarkers have been developed to improve the early identification and prognostication of patients with DKD. Novel biomarkers that capture one specific mechanism of the DKD disease process have been developed, and studies have evaluated the prognostic value of assay-based biomarkers either in small sets or in combinations involving multiple biomarkers. More recently, several studies have assessed the prognostic value of omics-based biomarkers that include proteomics, metabolomics, and transcriptomics. This review will first describe the biomarkers used in current practice and their limitations, and then summarize the current status of novel biomarkers for DKD with respect to assay-based protein biomarkers, proteomics, metabolomics, and transcriptomics.
Introduction
Diabetic kidney disease (DKD) is the leading cause of chronic kidney disease (CKD) and end-stage kidney disease (ESKD) worldwide [1]. Due to its association with a concomitant increase in cardiovascular morbidity and mortality, it remains one of the leading causes of reduced lifespan in people with diabetes mellitus (DM). Given the high risk of progressive deterioration in kidney function eventually leading to ESKD that requires kidney transplantation or chronic kidney replacement therapy, as well as increased risk of cardiovascular morbidity and mortality, early identification and risk stratification of disease is essential. Although our understanding of the pathophysiology of the disease has improved over the years, the prevalence of DKD has not changed significantly over the past 30 years [2].
To reduce disease prevalence and reverse or slow down disease progression, efforts to develop novel drugs have been ongoing, but many phase 3 clinical trials have failed to show any clinically significant findings [1,3]. For example, as oxidative stress is an important pathophysiological process in DKD, antioxidants have been developed to target the pathways of this disease. Although the antioxidant bardoxolone methyl (Reata Pharmaceuticals, Plano, TX, USA) showed promising phase 2 study results [4], administration of this agent in a phase 3 study showed an increased risk of early-onset fluid overload in patients with risk factors for heart failure [5]. Sulodexide, a purified mixture of sulfated glycosaminoglycan polysaccharides, can ameliorate DKD in animal experiments [6]. However, larger randomized controlled trials failed to demonstrate any beneficial clinical outcomes with the use of this agent [7,8]. As a result, efforts have been ongoing to develop novel biomarkers of DKD that can detect DKD at very early stages, as well as identify high-risk patients that are highly likely to eventually develop ESKD. Such novel biomarkers have also been developed to allow for risk stratification in clinical trials, as well as the development of drugs that specifically target these biomarkers.
This review will first describe current biomarkers used to predict the risk of DKD and disease progression, and then describe the current status of multiple novel biomarkers with respect to assay-based biomarkers, as well as omics-based biomarkers that include proteomics, metabolomics, and transcriptomics.
Biomarkers used in current practice
Markers of kidney function
The most commonly used current biomarkers of DKD are albuminuria and estimated glomerular filtration rate (eGFR) [9].
Given that albuminuria is an important component of DKD, as well as the strongest predictor of ESKD and cardiovascular morbidity in patients with type 2 DM [10], it is important to establish the degree of albuminuria in patients with DKD at the time of diagnosis. However, a major limitation of albuminuria as a biomarker of DKD is that not all patients with DKD have albuminuria. For example, approximately 30% of patients with DKD do not have albuminuria [11,12]. There is also a growing body of evidence suggesting that patients with type 1 or 2 DM can progress to ESKD in the absence of albuminuria, even after accounting for renoprotective agents [13–18]. In a recent study of 935 patients with type 1 DM and 1,984 patients with type 2 DM, followed for up to 16 years after the development of CKD stage 3, mean annual declines in eGFR for normo-, micro-, and macroalbuminuria for the first 10 years following the development of CKD stage 3 were 1.9, 2.3, and 3.3 mL/min/1.73 m2 in type 1 DM, and 1.9, 2.1, and 3.0 mL/min/1.73 m2 in type 2 DM, respectively [18]. In patients with normoalbuminuria, two distinct eGFR patterns were found, with one displaying an accelerated rate of eGFR decline. Of note, patients displaying this accelerated rate of eGFR decline were associated with less use of lipid-lowering treatment, renin-angiotensin system (RAS) blockers, and other antihypertensive treatments. These findings suggest that albuminuria has its limitations as a prognostic marker for DKD.
Current eGFR and past glomerular filtration rate (GFR) trajectory are well-established predictors of the future risk of ESKD [19]. Thus, eGFR is the most common prognostic biomarker used for predicting ESKD in both clinical practice and clinical trials. However, similar to albuminuria, eGFR also has important limitations as a prognostic biomarker of DKD. Limitations of using eGFR to predict DKD progression include different equations used to estimate eGFR, which include the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI), the Modification of Diet in Renal Disease (MDRD) equation, and eGFR calculated using cystatin C instead of creatinine [14]. The risk of DKD development or progression may be under or overestimated depending on which eGFR equation is used for risk stratification. For instance, in a study to assess population-based incidence rates of CKD in patients with DM depending on the eGFR equation, CKD incidence rates were higher when the MDRD equation, rather than the CKD-EPI equation, was used [20]. Moreover, considering that GFR is the product of the number of nephrons and the mean single nephron GFR, a reduction in the number of nephrons due to the progression of DKD can be compensated by an increase in the single nephron GFRs of surviving nephrons. Such changes may not be accurately reflected by the eGFR, as eGFR decline may only happen when each nephron exceeds its maximal filtration capacity. This is further confounded because the vasodilation of the afferent arteriole in patients with DKD may increase single nephron GFR even in the absence of nephron loss [21]. Thus, patients without actual functional nephron loss and those with actual functional nephron loss, but with compensation in GFR by remnant nephrons, may have identical eGFRs with vastly different prognoses.
As both albuminuria and eGFR have important limitations as prognostic biomarkers of DKD, the identification of novel diagnostic and prognostic biomarkers for the early risk stratification of DKD is much needed. Potential novel biomarkers for DKD are summarized in Table 1.

Summary of studies reporting on novel biomarkers for diabetic kidney disease (DKD)
Novel biomarkers of diabetic kidney disease—assay based
Considering the implications of the delayed identification of DKD progression, many studies have investigated potential predictive and prognostic biomarkers [22]. These biomarkers typically capture one specific aspect of the pathophysiology of the disease process such as tubular damage, inflammation, or oxidative stress [23]. However, given that DM is a heterogeneous disease involving multiple pathophysiological mechanisms, using just a single biomarker for the risk stratification of disease progression has several limitations. Single biomarkers have problems with individual, biological, and analytical variability. For example, novel biomarkers such as tissue necrosis factor receptor (TNFR) 1, TNFR2, fibroblast growth factor-23 (FGF-23), and high-density lipoprotein cholesterol are known to predict kidney outcomes in patients with type 2 DM [24–26]. However, TNFR1 and TNFR2 are not specific to type 2 DM, and measurements of FGF-23 may vary according to the choice of the analytical method [27]. Due to such issues, it is more likely that a panel of biomarkers will be needed to predict disease progression.
Single biomarkers or small sets of biomarkers—assay based
Single biomarkers typically capture a specific pathophysiological pathway of the DKD process, such as tubular damage, inflammation, oxidative stress, or endothelial dysfunction, whereas others focus primarily on glomerular features such as glycocalyx abnormalities, podocyte damage, or glomerular fibrosis.
Markers of tubular damage
Markers of tubular damage include kidney injury molecule-1 (KIM-1), neutrophil gelatinase-associated lipocalin (NGAL), and liver fatty acid-binding protein (L-FABP). Urinary concentrations of KIM-1, which is a protein expressed on the apical membrane of the proximal tubule cells, increase in response to acute kidney injury [28]. In a nested case-control study and a prospective cohort study, plasma KIM-1 levels were independently associated with a higher risk of eGFR decline in persons with early or advanced DKD [29]. Similarly, in a case-cohort study of 894 participants with DKD from the Chronic Renal Insufficiency Cohort (CRIC), higher plasma levels of KIM-1 were associated with an increased risk of DKD progression [30]. Another tubular marker that has been extensively studied is NGAL. NGAL is a 25-kDa protein from the lipocalin superfamily that was initially found in activated neutrophils but is also produced by kidney tubular cells in response to tubular injury. Higher levels of urinary NGAL have been shown to precede microalbuminuria in patients with type 1 DM [31,32]. In another study of 117 patients with type 2 DM, higher values of urinary NGAL have been observed in normoalbuminuric type 2 DM patients, and rose progressively in those with micro- and macroalbuminuria, suggesting that tubular damage may occur even in the very early stages of DKD [33]. Urinary L-FABP levels have also been shown to be associated with DKD progression. In patients with type 1 DM, high levels of urinary L-FABP predicted the initiation and progression of DKD and all-cause mortality, independent of the severity of albuminuria and other established risk factors [34]. In another cross-sectional and longitudinal study of 140 patients with type 2 DM without DKD and 412 healthy control subjects, urinary L-FABP levels accurately reflected the severity of DKD, and these levels were particularly high in those with normoalbuminuria [35]. High urinary L-FABP levels were found to be a strong and independent predictor of DKD progression [36].
Markers of inflammation
Biomarkers of inflammation such as tumor necrosis factor (TNF)-α and interleukin-1β (IL-1β) were first associated with DM in diabetic mouse models. Macrophages incubated with glomerular basement membranes produced significantly greater levels of both TNF-α and IL-1β than in nondiabetic mice [37]. This has led to further investigations into the use of TNF-α as a predictive marker of DM. Urinary TNF-α excretion and serum TNF-α levels were both found to be elevated in DKD [38]. Further investigations into the receptors that TNF-α bind to, namely TNFR1 and TNFR2, have also suggested that circulating TNFR levels could also be used as good predictors of DKD [24]. For example, in a cohort consisting of 349 patients with type 1 DM and proteinuria, TNFR2 levels were the strongest determinant of eGFR decline [39].
Another biomarker that captures the oxidative stress characteristics of the DKD pathophysiologic process is 8-hydroxy-2′-deoxyguanosine (8-OHdG), which is a product of oxidative DNA damage. It is excreted in the plasma and urine after the repair of DNA by nuclease [40]. This has led to the assessment of 8-OHdG as a biomarker of oxidative stress in patients with DM [41,42]. In two cohorts of patients with type 1 DM, higher plasma concentrations of 8-OHdG were independently associated with increased risk of kidney disease in individuals with type 1 DM, suggesting that this marker may be used to evaluate the progression of DKD [42]. However, in a study of patients with type 2 DM and healthy control subjects, although urine 8-OHdG levels were increased in patients with DM, its ability to predict the development of DKD was inferior to the urine albumin-to-creatinine ratio [43].
Markers of glomerular damage
In contrast to biomarkers that capture specific pathophysiological pathways of the DKD process, some well-known biomarkers, including transferrin, immunoglobulin G (IgG), IgM, and ceruloplasmin, reflect glomerular damage. In theory, as the molecular weight of transferrin is similar to that of albumin, urinary transferrin could also be a biomarker of DKD. In a study of 45 patients with type 2 DM and with normoalbuminuria or microalbuminuria, increased urinary transferrin levels in microalbuminuria patients significantly correlated with kidney biopsy-proven tubulointerstitial injuries, suggesting a potential role of urinary transferrin in the prediction of early tubular damage in patients with DKD [44]. In a more recent study of 60 patients with and without type 2 DM, urine transferrin correlated with subclinical atherogenesis in patients with type 2 DM without kidney dysfunction, suggesting that it could potentially be an early marker of endothelial dysfunction in patients with type 2 DM but without kidney dysfunction [45]. Another marker of glomerular damage that has been investigated is ceruloplasmin. Ceruloplasmin is a copper-carrying metalloenzyme that is more negatively charged than albumin, and thus is more difficult to be filtered by the glomerulus. In a study of 140 patients with type 2 DM with normoalbuminuria, urinary ceruloplasmin levels were found to be elevated in normoalbuminuric patients with DM and were highly predictive of the development of microalbuminuria [46]. Urinary IgM and IgG levels have also been shown to be predictive of DKD. A study of 22 patients with type 1 DM and 20 patients with type 2 DM, all with evidence of DKD, revealed that the increased urine excretion of IgG and IgM accompanied albuminuria in patients with type 2 DM, suggesting a potential role of urinary immunoglobulins in the risk stratification of DKD [47].
Multiple biomarkers—assay based
As DKD is a disease entity that involves multiple pathophysiological pathways, a combination of biomarkers may be required to accurately predict disease progression. For example, most studies that have investigated panels of candidate biomarkers have included TNFR, often in combination with biomarkers of tubular damage such as KIM-1 [29,30]. In a nested case-control of 380 participants, and a prospective cohort study of 1,156 participants with type 2 DM, higher plasma levels of KIM-1, TNFR-1, and TNFR-2 were associated with a higher risk of DKD progression, even after adjustments for age, relevant anthropometric, sociodemographic, and laboratory parameters. Of note, when all three plasma biomarkers were added to the clinical model, the area under the curve (AUC) for DKD progression improved from 0.680 to 0.752 [29]. A case-cohort study consisting of 894 participants with both type 1 and 2 DM reported similar findings, where higher levels of monocyte chemoattractant protein 1 (MCP-1) were also associated with a higher risk of DKD progression [30]. In a study of 260 Pima Indians with type 2 DM, urinary NGAL/creatinine was positively associated with risk of ESKD and mortality, whereas L-FABP/creatinine was inversely associated with ESKD. The addition of NGAL/creatinine and L-FABP/creatinine to models that included albuminuria and eGFR increased the C-statistics for predicting the risk of ESKD [48].
Other studies have explored higher numbers of potential candidate biomarkers to improve the prediction of DKD outcomes. In a study evaluating 17 potential urinary and seven plasma biomarkers in 67 participants with type 2 DM, urinary C-terminal FGF-23 was found to show the strongest association with ESKD, whereas plasma vascular endothelial growth factor (VEGF) was associated with the highest risk of the composite outcome of ESKD and death [49]. Another prospective study followed 83 patients with overt diabetic nephropathy and obtained repeated measurements of proteinuria, IL-1β, IL-6, IL-8, MCP-1, TNF-α, transforming growth factor-beta 1 (TGF-β1), and plasminogen activator inhibitor-1 (PAI-1) [50]. In the study, urinary MCP-1 and TGF-β1 predicted kidney function decline that was independent of albuminuria. In a more recent study involving 345 community-based patients with type 2 DM from the Fremantle Diabetes Study Phase II, eight potential candidate biomarkers were studied after adjustment for clinical parameters. Of these eight biomarkers, apolipoprotein A4 (apoA4), CD5 antigen-like (CD5L), and complement C1q subcomponent subunit B (C1QB) were independently associated with the rapid decline in kidney function, improved predictive performance, fitness, discrimination, and reclassification [51].
However, as evidenced in the SUMMIT (the Surrogate Markers for Micro- and Macro-Vascular Hard Endpoints for Innovative Diabetes Tools) program [52], there are very strong correlations between these biomarkers, and this confounds the interpretation of these biomarkers as predictors of disease progression. Further optimization of a panel of best-reported biomarkers would be needed. Ideally, future studies could explore a panel of biomarkers that show low correlation with each other. Moreover, most studies reported to date are small in sample size, and therefore studies consisting of larger populations would be needed for the validation of the aforementioned biomarkers.
Novel biomarkers of diabetic kidney disease—omics based
The omics platform-based approach
Over the last decade, the use of approaches that measure large sets of lipids, metabolites, amino acids, peptides, and proteins are increasing [53]. These approaches have been called omics-based tests, and are defined as an assay derived from multiple molecular measurements that allow the quantification of all RNAs, proteins, and metabolites present in biological samples, and interpreted by computational models to produce clinically meaningful results. Omics-based approaches have the advantage of not only measuring a full spectrum of peptides or metabolites in a short amount of time but also producing large sets of unbiased data that can be used for diagnosis, prediction of disease progression, and treatment response. As a result, this omics platform-based approach has emerged as a strong tool in biomarker discovery in recent years [53] (Fig. 1).
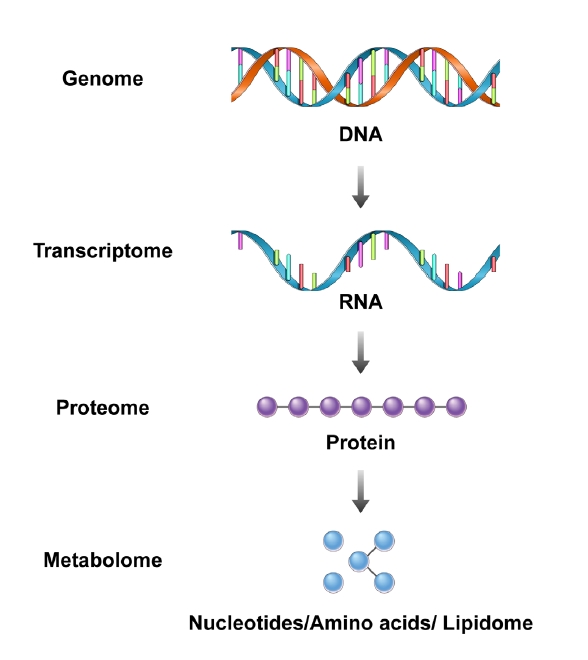
The concept of the omics platform-based approach consists of the genome, transcriptome, proteome, and metabolome.
Proteomics
Proteomics allows the simultaneous quantification of multiple protein markers in a biological sample [54,55]. Although tissue samples provide the most information on protein expression, DKD is often diagnosed clinically, rather than by biopsy, and therefore the number of patients who will undergo kidney biopsy for DKD will not increase. Blood samples can display protein signals that are produced from the kidney and of more generic processes such as fibrosis [56]. However, obtaining large volumes of blood samples in patients is often not feasible. The collection of urine samples overcomes the limitations of blood samples. Urine collection is not only available in large volumes, but it is also noninvasive. This led to urinary proteomics gaining more attention as a tool for the identification of diagnostic and prognostic biomarkers in kidney disease [57].
Early studies using proteomics in DKD used urinary samples to improve early diagnosis and the prediction of kidney-related and other outcomes [58–60]. The most studied and well-validated proteomic classifier to date is the capillary electrophoresis-mass spectrometry-based urinary peptide classifier, CKD-273. This mass spectrometry-based method combines the data of 273 urinary peptides into a combined score that has high accuracy in predicting the new onset of albuminuria. Approximately 75% of the peptides are collagen fragments, with uromodulin, clusterin, albumin, β-2 microglobulin, α-1 antitrypsin, and others comprising the remainder. The diagnostic utility of this proteomic classifier was first developed in a cross-sectional study of 3,600 patients with different CKD etiologies, where the classifier showed a sensitivity of 85% and a specificity of 100% for the diagnosis of CKD [61].
This classifier was subsequently validated across several cohorts consisting of patients with type 2 DM, where CKD-273 predicted both the development and progression of albuminuria in patients with DKD. In a prospective study of 35 patients with either type 1 or 2 DM, CKD-273 was able to predict progression to macroalbuminuria 5 years before the actual onset [62]. In another prospective case-control study from the PREVEND (Prevention of Renal and Vascular End-stage Disease) study and from the Steno Diabetes Center (Gentofte, Denmark), the proteomic classifier was independently associated with the transition to micro- or macroalbuminuria. The classifier improved the predictive ability of albuminuria and eGFR in the development and progression of albuminuria [63]. Analyses of both the Effect of Candesartan on Progression of Retinopathy in Type 1 Diabetes (DIRECT-Protect 1) and in Type 2 Diabetes (DIRECT-Protect 2) studies demonstrated that the CKD-273 classifier was able to predict microalbuminuria, independent of treatment, age, sex, systolic blood pressure, albuminuria, eGFR, hemoglobin A1c (HbA1c), and DM duration [60,64–66]. More recently, in a study of 1,014 individuals with type 1 or 2 DM, baseline eGFR of ≥70 mL/min/1.73 m2, and normoalbuminuria, CKD-273 was able to identify patients with DM who will progress to eGFR of <60 mL/min/1.73 m2 in the absence of albuminuria, independent of age, blood pressure, and baseline eGFR [67]. The concept that CKD-273 may be useful in determining the risk of disease progression and that it may also stratify treatment response to spironolactone was more definitively tested in the recent PRIORITY (Proteomic Prediction and Renin Angiotensin Aldosterone System Inhibition Prevention of Early Diabetic nephropathy in Type 2 Diabetic Patients with Normoalbuminuria) trial. In 1,775 participants with type 2 DM and normoalbuminuria over a median follow-up time of 2.5 years, high-risk patients defined by CKD-273 were more likely to develop microalbuminuria, even after adjustments for baseline risk factors such as HbA1c, systolic blood pressure, baseline albuminuria, and eGFR [68]. However, spironolactone did not prevent progression to microalbuminuria in high-risk patients. On the contrary, in an exploratory analysis of the MARLINA-T2D (Efficacy, Safety & Modification of Albuminuria in Type 2 Diabetes Subjects With Renal Disease With LINAgliptin) trial, where participants were randomized to receive either linagliptin or placebo for 24 weeks, there was a significant correlation between CKD-273 and clinical renal parameters as well as eGFR decline. Patient stratification using this classifier found that linagliptin had the potential to slow progressive kidney function decline in high-risk CKD patients [69].
Results from urinary proteomic studies have improved our knowledge of the pathophysiology of DKD. Other proteomic methods include the use of collagen fragments. For example, the α1 type 1 collagen chain is significantly altered in urine 3 to 5 years before the onset of macroalbuminuria [62]. It was found that before urinary albumin excretion starts to increase, urinary collagen fragments decreased. In a multicenter study involving 165 patients with type 2 DM, type I and type III α1 collagen and α2-Heremans-Schmid-glycoprotein were found to be prominent collagen markers. Therefore, it is thought that collagen fragments originate from the kidney, and a decrease in these fragments in patients with DKD may be due to the accumulation of extracellular matrix and increased kidney fibrosis [70].
Other urinary peptides that have been studied include uromodulin, progranulin, clusterin, α1 acid glycoprotein, and haptoglobin. In a nested case-control design, a panel including uromodulin, progranulin, clusterin, and α1 acid glycoprotein predicted an early decline in eGFR in a cohort of 465 adults with type 1 DM [71]. Moreover, in a study of patients with DKD from the VADT (Veterans Affairs Diabetes Trial), urinary haptoglobin was identified as a candidate biomarker to predict early kidney functional decline [72].
Regardless of which sample is used for proteomic analysis, the use of proteomics to predict DKD development and progression still has several limitations including the absence of well-validated diagnostic criteria. Prospective validation studies are needed before the widespread implementation of proteomics in DKD.
Metabolomics
Metabolomics is the measurement of low-weight intermediates (<500 Da) and small end products of biochemical processes in biological fluids, and they have emerged as another potential tool in the discovery of novel biomarkers for kidney diseases. The metabolome is often regarded as the final downstream integration of biological information that consists of the genome, proteome, transcriptome, and overall enzymatic reactions of an individual [73]. This enables the detection of short- and long-term physiological and pathological changes that occur in chronic diseases. However, their results are often difficult to interpret due to various confounders that include lifestyle, medications, and nutritional status [74].
Metabolites may originate from blood or urine. Plasma nonesterified and esterified fatty acids were found to differentiate albuminuria stages in patients with type 2 DM [75]. In a study of 78 diabetic patients, a combination of serum metabolites with multivariate analyses enabled accurate discrimination of patients with DKD. In the study, the selection of five metabolites that included γ-butyrobetaine, symmetric dimethylarginine, azelaic acid, and two unknowns yielded an AUC value of 0.927 for diagnosing DKD [76]. Another study that included healthy controls and patients with type 2 DM indicated that serum metabolite levels of leucine, dihydrosphingosine, and phytosphingosine were significantly different in these two patient groups [77]. In the SUMMIT study, a combination of biomarkers of tubular damage such as KIM-1 and β2-microglobulin, and metabolite markers were used to predict the rapid progression of DKD in individuals with type 2 DM. A total of 207 serum biomarkers were measured, of which 12 biomarkers showed significant associations with rapid progression, all adjusted for clinical characteristics. A combination of 14 serum biomarkers increased the predictive ability. The addition of biomarkers to clinical data improved baseline AUC from 0.706 to 0.868. Biomarkers in the predictive model included fibroblast growth factor-21, the symmetric to asymmetric dimethylarginine ratio, β2-microglobulin, C16-acylcarnitine, and KIM-1 [78].
Urine metabolites that have been studied to date include octanol, oxalic acid, phosphoric acid, benzamide, creatinine, 3,5-dimethoxymandelic amide, and N-acetylglutamine [79]. One study combined both plasma and urinary metabolites to improve the predictive utility of metabolites. In a study of 90 patients with type 2 DM, urine hexose, glutamine, tyrosine, plasma butenoylcarnitine, and histidine levels predicted the development of albuminuria, independent of baseline albuminuria levels, eGFR, and use of RAS blockers [80]. In a study from the CRIC consisting of 1,001 participants with DM and CKD, after adjustments for clinical variables, urinary 3-hydroxyisobutyrate (3-HIBA) and 3-methylcrotonyglycine levels had a significant negative association with eGFR slope, whereas aconitic and citric acid levels showed a positive association. Levels of 3-HIBA and aconitic acid were each associated with higher and lower risks of ESKD requiring kidney replacement therapy, respectively [81]. Most recently, in 2,670 patients with type 1 DM from the Finnish Diabetic Nephropathy study, seven urinary metabolites, which included leucine, valine, isoleucine, pseudouridine, threonine, and citrate, were associated with DKD progression after adjustment for baseline albuminuria and CKD stage. Moreover, 2-hydroxyisobutyrate was associated with the progression of DKD in individuals with normoalbuminuria, and six amino acids and pyroglutamate were associated with the progression of DKD in those with macroalbuminuria [82].
Although there have been significant advances in the field of metabolomics for patients with DKD, most of the aforementioned studies are cross-sectional. Not only is there a need for more prospective studies to evaluate the predictive utility of these metabolites, but replication of current findings in other cohorts is also needed to convey therapeutic targets and improve the clinical management of DKD.
Transcriptomics
Transcriptomic studies of DKD use micro RNAs (miRNAs), which are small non-coding RNAs that block protein translation and can induce messenger RNA degradation. Thus, miRNAs are regarded as regulators of gene expression. Like metabolites, miRNAs may also originate from plasma, serum, or urine, and their profiling can be performed using either traditional microarray/real-time polymerase chain reaction (RT-PCR) platforms or RNA sequencing.
One of the earliest studies to indicate that certain plasma miRNAs showed an association with the progression of DKD was performed in patients with type 1 DM with albuminuria but normal kidney function. In participants of the Joslin cohort, baseline circulating TGF-β1-regulated miRNA levels were associated with progression to ESKD requiring kidney replacement therapy. Baseline miRNA levels of let-7c-5p and miR-29a-3p were independently associated with more than a 50% reduction in the risk of progression to ESKD, whereas baseline miRNA levels of let-7b-5p and miR-21-5p were associated with a more than 2.5-fold increase in the risk of ESKD [83]. In another cross-sectional nested case-control study from the EURODIAB Prospective Complications Study of 455 patients with type 1 DM, miR-126 levels were negatively associated with all DM-related complications. Although this association was no longer significant after adjustment for both hyperglycemia and duration of DM, a statistically significant 25% risk reduction of proliferative diabetic retinopathy was observed even after adjustments for HbA1c and DM duration [84].
In addition to miRNAs sampled from the plasma or serum, many studies have reported findings from urine samples. One of the earliest studies to report on the association between urinary miRNAs and the risk of DKD progression was conducted with 83 patients with type 2 DM, where baseline urinary miRNA levels of miR-29a and miR-29b were associated with complications of DM. Higher levels of urinary miR-29a were observed in patients with albuminuria compared to those with normoalbuminuria. Urinary miR-29a levels showed a significant correlation with albuminuria and were also correlated with carotid intima-media thickness [85]. Another study assessed the urinary extracellular vesicle (EV)-miRNA profiles of patients with type 1 DM, where 22 of 377 urinary EV-miRNAs were differentially expressed in patients with normoalbuminuria compared to albuminuric patients. Results showed that miR-130a and miR-145 were enriched, whereas miR-155 and miR-424 were reduced in urinary exosomes for patients with albuminuria [86]. More recently, in a study of 209 patients with biopsy-proven DKD, urinary miR-196a levels correlated positively with proteinuria, duration of DM, and systolic blood pressure, whereas baseline eGFR and hemoglobin levels showed a negative correlation with urinary miR-196a. This suggests that increased urinary miR-196a levels were significantly associated with the progression of DKD and could be a noninvasive prognostic marker of kidney fibrosis in patients with DKD [87].
Although several other studies have investigated transcriptomics in patients with DKD, there is no overlap in the specific miRNAs being reported as being relevant to DKD. It is most likely that a combination of miRNAs may be needed for the early detection of DKD rather than a single miRNA [88]. Therefore, the evidence to support a clinically useful role of miRNAs in the early diagnosis and risk stratification of DKD remains uncertain.
Current practice and conclusion
Current treatment of DKD relies on lifestyle modification, and medication that controls hyperglycemia, hypertension, and proteinuria. However, even the optimal implementation of this strategy often fails to prevent progression to ESKD in a substantial proportion of patients. There is hope that novel biomarkers, both assay-based and omics-based, will help to identify patients at the highest risk and guide the treatment of these patients. In reality, only a few trials use biomarkers other than albuminuria or eGFR to enroll and risk stratify study participants [89], and even fewer studies assess the effect of treatments with novel biomarkers [90–92]. In part, this may be because potential novel biomarkers only modestly improve the performance of eGFR and albuminuria, which are the biomarkers currently available. Moreover, considering that the progression of DKD is usually a slow process that may take decades to emerge, the setting of robust clinical endpoints in clinical trials is often not feasible.
Although the novel biomarkers discussed in this review have enormous potential in the field of DKD, future studies should look into using these biomarkers either as enrolment criteria for randomized clinical trials or as surrogates of study endpoints. Larger study cohorts with kidney biopsies and both urine and plasma or serum samples from the same patients would also be needed. To obtain comparable and reproducible data, consensus protocols for sample collection, processing, and analysis should be defined across collaborators. Finally, as we gain a deeper understanding of the DKD pathophysiology, an increasing number of potential novel biomarkers will be available. To improve the prognostication of patients with DKD, it will be essential to integrate these novel findings and biomarkers into the design of future clinical trials.
Notes
Conflicts of interest
Tae-Hyun Yoo is the Editor-in-Chief of Kidney Research and Clinical Practice and was not involved in the review process of this article. All authors have no other conflicts of interest to declare.
Funding
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (NRF-2020R1F1A1049799).
Authors’ contributions
Writing–original draft: CYJ
Writing–review & editing: THY
All authors read and approved the final manuscript.
Acknowledgements
The authors thank the Medical Illustration & Design team of the Medical Research Support Services of Yonsei University College of Medicine for all artistic support related to this work.