



Introduction
Chronic kidney disease-associated pruritus (CKD-aP), also known as uremic pruritus, is defined as itching that is directly related to kidney disease without other comorbidities that could cause the itching. It usually presents as itching across large bilaterally symmetrical surface areas without a dermatomal pattern, with daily or near-daily occurrence [1]. In addition, it can manifest as localized itching on the back, face, or arms [2,3]. CKD-aP causes adverse effects on sleep quality, mood, and social functions and is independently associated with mortality [2,4]. Although its pathophysiology is incompletely understood, the known predisposing factors for its development include increased blood urea nitrogen, hyperphosphatemia, and hyperparathyroidism [5–7]. Other contributing factors include anemia, elevated ferritin, low transferrin, and low albumin levels [8]. Therefore, although the mechanisms of CKD-aP are poorly understood, metabolic disequilibrium as a result of renal failure could be a cause.
Despite advances in hemodialysis patient care during the past few decades, CKD-aP remains a major clinical symptom and medical challenge. Resistant pruritus is defined as an itch lasting >4 weeks despite adequate dialysis, optimization of metabolic parameters, and the use of topical emollients and analgesics [9]. Such patients can be treated with oral antihistamines; if pruritus persists after 1 to 2 weeks of that treatment, they can be treated with gabapentin or pregabalin. Most patients with CKD-aP partially respond to emollients, topical analgesics, oral antihistamines, or gabapentin [9]. For patients who are refractory to these agents, narrowband ultraviolet B (NB-UVB) phototherapy is an effective therapeutic choice [9]. The benefits of NB-UVB phototherapy are thought to occur through modulation of the inflammatory state of these patients [10]. However, only small or uncontrolled clinical studies have been conducted on the effect of NB-UVB phototherapy on CKD-aP.
A low serum vitamin D level is associated with the metabolic disequilibrium commonly observed in patients undergoing hemodialysis [11,12], possibly because of reduced skin synthesis of vitamin D [13]. These patients are likely exposed to less sunlight than average [14,15], and uremia can blunt the response of serum vitamin D to ultraviolet B (UVB) irradiation [13]. Moreover, hyperpigmentation, a common cutaneous manifestation in these patients, could play an additional role in impairing the endogenous synthesis of vitamin D [14,16]. Therefore, NB-UVB phototherapy could be a way to improve the serum vitamin D balance in patients undergoing hemodialysis. Ala-Houhala et al. [17] showed that NB-UVB phototherapy significantly improved serum vitamin D balance in these patients. Meanwhile, inflammatory skin disease is related to low serum vitamin D levels [18,19]. Additionally, vitamin D supplementation reduces disease activity in patients with inflammatory skin disease [20–23]. Taken together and considering CKD-aP as a skin counterpart of chronic inflammation in patients undergoing hemodialysis [24], the benefit of NB-UVB phototherapy on CKD-aP might correlate with improved serum vitamin D levels.
As an effective treatment choice for refractory CKD-aP, NB-UVB phototherapy has been postulated to improve serum vitamin D levels, in addition to modulating the inflammatory state. However, data on serum vitamin D levels and NB-UVB phototherapy in CKD-aP are lacking. Therefore, we investigated the degree of CKD-aP amelioration and changes in serum vitamin D levels after NB-UVB phototherapy in patients undergoing hemodialysis.
Methods
Ethics statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Review Board of Kangdong Sacred Heart Hospital (No. 2018-01-008). Written informed consent was obtained from all patients prior to enrollment. This study was registered at Clinical Research Information Service (http://cris.nih.go.kr; KCT0003701).
Patients
This study was conducted at Kangdong Sacred Heart Hospital between March 2018 and December 2020. The inclusion criteria were as follows: 1) age of >18 years; 2) undergoing hemodialysis thrice a week for >3 months; 3) amount of dialysis delivered (Kt/Vurea; K = clearance of urea, t = time on dialysis, V = estimated total body water) of >1.2; 4) hemoglobin (Hb) level of >10 g/dL; 5) pruritus with an intensity of ≥5 measured on a visual analog scale (VAS); 6) pruritis for ≥2 months; and 7) no response to oral antihistamines, gabapentin or pregabalin, or topical emollients. Of note, if the pruritus did not improve after 4 weeks of topical emollients, patients took oral antihistamines for 2 weeks. After that, the patients whose pruritus did not improve took gabapentin or pregabalin for 2 weeks. If the pruritus still did not improve, it was defined as no response. The exclusion criteria were a history of photosensitivity, active infection, psychotic illness or other communication disability, primary skin disorder, cholestatic liver disease or acute hepatitis, and active malignancy.
Phototherapy and protocol
NB-UVB phototherapy was administered to the whole body surface in an ultraviolet irradiation cubicle (HOUVA-II; National Biological Corp.) incorporating Phillips TL-01 lamps with a peak wavelength emission of 311 nm. Phototherapy was conducted thrice weekly for 12 weeks, for a total of 36 sessions. The initial dose of NB-UVB was 280 mJ/cm2, which is approximately 70% of the minimal erythema dose. The phototherapy dose was generally increased by 10% to 15% per session, as tolerated. According to the response, the phototherapy dose was adjusted as follows: maintaining the previous dose if asymptomatic erythema appeared for 24 hours; reducing the dose by 10% if erythema was accompanied by mild pain or pruritus; restarting from one-third of the dose after recovery if painful erythema or bullae formation associated with mild pain or pruritus occurred.
Study design, data collection, and outcome measures
This was a before-and-after study design. At baseline, we evaluated the intensity of the pruritus using the VAS score (0 [no pruritus] to 10 [most severe pruritus]). The VAS score was evaluated each time the patients received NB-UVB phototherapy. Laboratory parameters of serum Hb, ferritin, transferrin saturation (TSAT), intact parathyroid hormone (iPTH), 25-hydroxy vitamin D [25(OH)D], calcium, phosphate, C-reactive protein (CRP), and Kt/V values were measured at baseline and after 12 weeks. If the patient did not complete the phototherapy protocol, laboratory parameters were measured at the next dialysis session after the end of phototherapy.
Vitamin D deficiency and insufficiency were defined as serum 25(OH)D concentrations of <20 ng/mL and 20–30 ng/mL, respectively. The Δ25(OH)D was calculated as the difference between the serum 25(OH)D concentration at 12 weeks or the last follow-up day and that at baseline. The response of CKD-aP to NB-UVB phototherapy was assessed by the change in the intensity of pruritus over time, with rapid response defined as a reduction in the VAS score of ≥50% within the first 6 weeks.
Statistical analysis
Statistical analyses were performed using IBM SPSS version 27.0 (IBM Corp.) and R version 3.6.1 (R Foundation for Statistical Computing). Differences before and after NB-UVB phototherapy were analyzed using the Wilcoxon signed-rank test. Continuous variables are expressed as means ± standard deviations, and categorical variables are expressed as numbers (percentages). Differences between groups were assessed using Student t test, the chi-square test, or Fisher exact test. Changes in VAS scores over time were compared between groups using a linear mixed model analysis. A logistic regression analysis was performed to assess variables associated with a rapid response. A multivariate analysis was performed using all covariates with p-values of <0.1 in the univariate analyses. Even if their p-values were >0.1, potential confounding factors were included in the multivariate analysis. All probabilities were two-tailed, and statistical significance was set at p < 0.05.
Results
Study patients
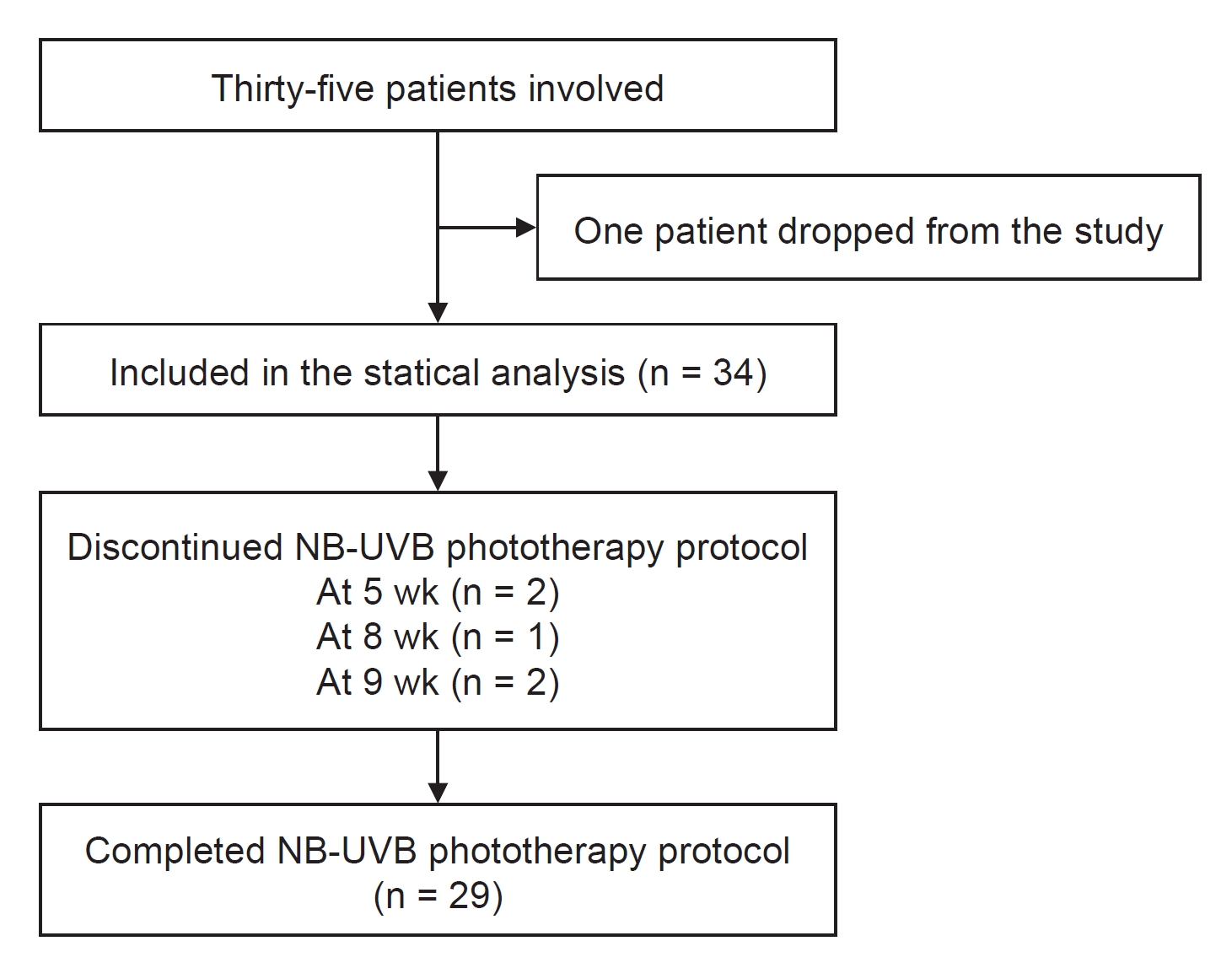
Initially, 35 patients enrolled in the study. One patient dropped out immediately (after the first session) because she could not tolerate the heat in the cabinet during phototherapy. Therefore, 34 patients with at least one follow-up visit were included in the statistical analyses. Two and three patients withdrew from the phototherapy protocol within 6 weeks and after 6 weeks, respectively. Thus, 29 patients completed the phototherapy protocol. None of the withdrawals were due to a lack of efficacy. A flowchart of the patients is shown in Fig. 1.
Narrowband ultraviolet B phototherapy and change in serum vitamin D
Prior to NB-UVB phototherapy, the median serum 25(OH)D concentration was 10.9 ng/mL (interquartile range [IQR], 5.3–26.0 ng/mL) in all patients. Among them, 23 and 8 patients had vitamin D deficiency and insufficiency, respectively. After the last NB-UVB phototherapy session, the median serum 25(OH)D concentration was 32.5 ng/mL (IQR, 25.8–39.3 ng/mL). That increase was statistically significant (p < 0.001), and the serum 25(OH)D concentration increased by a median of 17.4 ng/mL (IQR, 11.0–22.4 ng/mL). At that time, four and seven patients had vitamin D deficiency and insufficiency, respectively. Notably, serum iPTH and calcium concentrations did not change after the NB-UVB phototherapy course. In addition, the serum Hb, ferritin, TSAT, phosphate, CRP, and Kt/V values were unchanged (Table 1).
Baseline characteristics according to the change in serum vitamin D
The subjects’ median age was 62 years (IQR, 56–69 years), and 14 patients (41.2%) were male. The median dialysis duration was 52.5 months (IQR, 29.6–107.4 months). The underlying cause of end-stage renal disease (ESRD) was diabetes in 23 patients (67.6%). Notably, none of the patients required nutritional vitamin D. When the patients were divided into two groups according to the median Δ25(OH)D level, serum iPTH concentrations were significantly higher in patients with Δ25(OH)D of ≤17.4 ng/mL than in those with Δ25(OH)D of >17.4 ng/mL. However, the groups did not differ with respect to age, sex, dialysis duration, underlying cause of ESRD, VAS score, cumulative dose of NB-UVB phototherapy, serum Hb concentration, ferritin concentration, TSAT, 25(OH)D concentration, calcium concentration, phosphorus concentration, CRP level, or Kt/V. To control secondary hyperparathyroidism, 13 patients used synthetic vitamin D analogues (calcitriol in eight and paricalcitol in five). The proportion of patients receiving synthetic vitamin D analogues did not differ between patients with Δ25(OH)D of ≤17.4 ng/mL and those with Δ25(OH)D of >17.4 ng/mL (Table 2). Of note, not all patients used vitamin D supplementation.
Response to narrowband ultraviolet B phototherapy according to the change in serum vitamin D
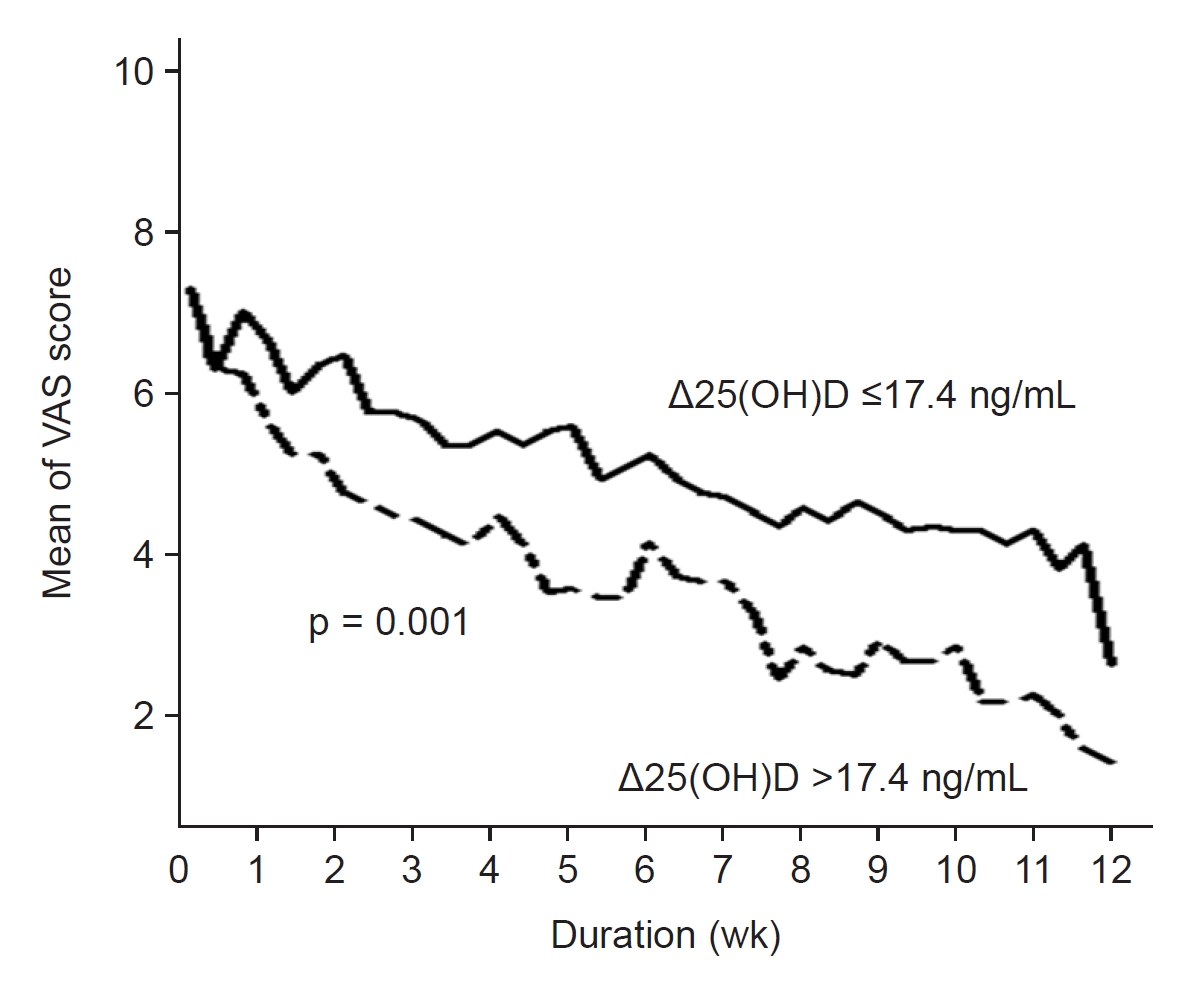
NB-UVB phototherapy reduced the VAS score for pruritus intensity more significantly in patients with Δ25(OH)D of >17.4 ng/mL than in patients with Δ25(OH)D of ≤17.4 ng/mL (p = 0.001) (Fig. 2). Notably, NB-UVB phototherapy significantly improved the VAS score for pruritus intensity over time in all patients (p < 0.001) (Fig. 2). Among them, 10 exhibited a rapid response. The logistic regression analysis showed that Δ25(OH)D was independently associated with a rapid response (odds ratio [OR], 1.20; 95% confidence interval [CI], 1.05–1.38; p = 0.01). The effect of Δ25(OH)D on rapid response remained significant even after adjustment for levels of serum Hb, ferritin, TSAT, iPTH, 25(OH)D, calcium, phosphate, CRP, and Kt/V (OR, 1.29; 95% CI, 1.02–1.63; p = 0.04) (Table 3).
Discussion
This pre–post clinical study investigated the degree of CKD-aP amelioration according to changes in serum vitamin D levels after NB-UVB phototherapy in patients undergoing hemodialysis. Similar to previous studies, we found that NB-UVB phototherapy was an effective treatment for CKD-aP. We also found that the change in serum 25(OH)D concentration after NB-UVB phototherapy correlated significantly with rapid improvement of refractory CKD-aP.
CKD-aP is considered to be a systemic rather than a local skin disorder [24,25]. Various serological parameters have been identified as potential pruritogens in chronic kidney disease. Parathyroid hormone (PTH) is a possible pathogenic serologic parameter based on the observation that persistent pruritus improves after parathyroidectomy in patients with secondary hyperparathyroidism [6,7]. In addition, hypercalcemia and hyperphosphatemia with secondary calcium phosphate crystal deposits in the skin are possible mechanisms [26]. However, PTH did not elicit any cutaneous reaction upon intradermal application in humans, and it was not detected in skin biopsies of affected patients [27]. In addition, little clinical evidence supports an association between CKD-aP and higher calcium and phosphate levels [17]. Interestingly, Gilchrest et al. [28] showed that the response of CKD-aP to UVB phototherapy was unaffected by secondary hyperparathyroidism. In line with those findings, we found that a rapid response to NB-UVB phototherapy in refractory CKD-aP did not correlate with iPTH, calcium, or phosphate levels.
Systemic inflammation might play a role in CKD-aP [24,25]. Serological inflammatory parameters, including increased white blood cell count, low albumin level, and high ferritin level, are reportedly associated with CKD-aP [8,29]. In addition, an experimental study showed that UVB radiation could modulate the immune system [10]. Interestingly, Gilchrest et al. [30] showed that tanning patients with UVB phototherapy led to CKD-aP relief, and the effect was maintained even when only half of the body was irradiated. Taken together, these findings suggest that UVB radiation has a systemic effect in modulating the inflammatory state of CKD-aP. In this study, NB-UVB phototherapy significantly reduced CKD-aP intensity. However, the serum ferritin and CRP concentrations did not change after the course of NB-UVB phototherapy. In addition, rapid response to NB-UVB phototherapy in refractory CKD-aP did not correlate with ferritin or CRP levels.
Special attention has been focused on imbalances in the expression of mu (μ)- and kappa (κ)-opioid receptors, which cause pruritus [31,32]. Thus, pruritus is increased by μ-receptor activation and κ-receptor blockade and decreased by κ-receptor activation and μ-receptor blockade [33]. This opioid hypothesis is supported by the observation that the ratio of the μ-receptor agonist (beta-endorphin) to the κ-receptor agonist (dynorphin-A) is higher in hemodialysis patients than in healthy controls, and this ratio increases with the severity of pruritus [34]. Meanwhile, UVB light is reportedly responsible for the formation of vitamin D-generated beta-endorphin [35–37]. Therefore, the opioid hypothesis cannot explain the effect of NB-UVB therapy on CKD-aP.
Recent research on CKD-aP points toward the dysregulation of cutaneous innate immunity. Vitamin D plays an important role in the cutaneous innate immune response by regulating the production of the antimicrobial peptide cathelicidin, which is associated with the complex pathogenesis of several chronic inflammatory skin diseases [38]. In addition, vitamin D is considered to be a calcium-regulating hormone in the skin because it regulates the calcium gradient, which is essential for keratinocyte differentiation, in the upper layers of the skin [39]. Momose et al. [40] demonstrated that disruption of the calcium gradient in the upper layers of the skin was associated with CKD-aP. Therefore, vitamin D might adjust the abnormal calcium gradient and consequently regulate abnormal keratinocyte differentiation and reduce the xerosis commonly observed in the skin of CKD-aP patients. Although the precise mechanisms to explain the association between vitamin D and CKD-aP have not been established, the function of vitamin D on keratinocytes might also be related to the underlying pathogenesis. Several clinical studies have shown that patients with inflammatory skin disease have significantly lower serum vitamin D levels than controls [18,19]. In addition, a high dose of vitamin D supplementation reduces disease activity in patients with inflammatory skin disease [20–23].
Vitamin D can be generated in the skin during exposure to sunlight or obtained from diet and supplements. Sun exposure is the primary source of vitamin D in humans. Specifically, the UVB portion of natural sunlight (spectral range, 290–320 nm) generates previtamin D from 7-dehydrocholesterol (provitamin D) in the upper layers of the skin. That previtamin D undergoes a slow temperature-dependent thermal isomerization into vitamin D. Vitamin D is then metabolized into 25(OH)D in the liver [41]. Indeed, several clinical studies have shown that both artificial UVB sources, broadband-UVB and NB-UVB, can lead to 25(OH)D synthesis [17,41–43]. Interestingly, in this study, rapid improvement of refractory CKD-aP after UVB phototherapy correlated significantly with Δ25(OH)D.
Our study has several limitations. First, similar to other clinical studies on CKD-aP, this study was small and uncontrolled. However, we are the first to evaluate the degree of CKD-aP amelioration based on changes in serum vitamin D levels after NB-UVB phototherapy in patients undergoing hemodialysis. Second, this study would have been much more persuasive if we had used other scales, such as the Pruritus Numerical Rating, Peak Pruritus Numerical Rating, Worst Itch Numeric Rating, or 0–21-point itch severity, instead of the VAS to measure pruritus intensity. Third, we did not perform a skin biopsy to evaluate changes in microinflammation and vitamin D in the skin of patients with CKD-aP before and after the course of NB-UVB phototherapy. Fourth, based on the opioid hypothesis, measures of beta-endorphin and dynorphin-A are required to explain the effect of NB-UVB phototherapy on CKD-aP; this study did not measure those parameters.
Despite those limitations, this study has shown that the effect of NB-UVB phototherapy on CKD-aP might correlate with improved serum vitamin D levels. Further well-designed clinical and experimental studies are needed to clarify the relationship between NB-UVB phototherapy and serum vitamin D levels in CKD-aP patients.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









