The effect of depression and health-related quality of life on the outcome of hemodialysis patients☆
Article information
Abstract
Background
In hemodialysis (HD) patients, traditional risk factors cannot explain all of the mortality and morbidity. This study was designed to investigate the effect of depression and health-related quality of life (HRQOL) on prognosis in maintenance HD patients.
Methods
In February 2008, the Beck's Depression Inventory and the Kidney Dialysis Quality of Life—Short Form were utilized to measure depression and HRQOL. Until February 2011, the mortality, cardiovascular events, infection, and hospitalization were investigated, retrospectively.
Results
Among the 166 patients, the 3-year cumulative survival rate was 88.8%, and the depression did not affect survival (depression vs. nondepression: 91.8% vs. 87.2%, P=0.437). The upper tertiles in physical component summary (PCS) were correlated with lower mortality (OR, 0.12; P=0.05) and fewer cardiovascular events (OR, 0.09; P=0.024) than the lower tertiles. The upper tertiles in kidney disease component summary (KDCS) were associated with less hospitalization than the lower tertiles (OR, 0.38; P=0.024). After adjusting for multiple variables including age, comorbidity index, and albumin, upper tertiles in PCS were correlated with fewer cardiovascular events than the lower tertiles (OR, 0.08; P=0.038).
Conclusion
The cross-sectional survey of whether HD patients had depression was not significantly associated with mortality and morbidity. HRQOL was correlated with mortality, cardiovascular events and hospitalization.
Introduction
In hemodialysis (HD) patients, traditional risk factors including diabetes mellitus, atherosclerosis, and smoking, significantly worsen prognosis of patients; however, these factors cannot explain all of the mortality and morbidities of the HD patients. Depression is the most common psychological problem among end-stage renal disease (ESRD) patients [1]. The health-related quality of life (HRQOL), which reflects patients' subjective “well-being”, as well as depression is related to higher morbidity and mortality rates in HD patients [2], [3], [4]. However, the studies about the effect of depression and HRQOL on the HD patients' mortality and morbidity in Korea are scarce. The aim of this study was to investigate the effect of depression and HRQOL on patients' prognosis in maintenance HD patients.
Methods
Patients and methods
We have previously described the methods for evaluating depression and HRQOL of patients [5]. A total of 166 ESRD patients on maintenance HD from three university hospitals (Seoul National University Hospital, Seoul National University Bundang Hospital, Seoul National University Boramae Hospital) and three local dialysis clinics in Seoul were included. These participants had been on a HD program for more than 3 months before study recruitment. Exclusion criteria were those patients who had started dialysis for acute kidney injury or who had been on dialysis for less than 3 months. Patients who refused to enroll were excluded from this study. We also excluded patients who were diagnosed with dementia. Interviewers read and checked the questionnaires for the patients who had difficulty in reading and writing. The Beck's depression Inventory (K-BDI) and the Korean version of Kidney Dialysis Quality of Life—Short Form (KDQOL-SFTM) were utilized to measure depression and HRQOL in maintenance HD patients at February 2008. The BDI contains 21 self-reported items which are rated on a scale of 0–3 points [6]. To define moderate to severe depression as a depression group, we established 18 as a cut-off value. Furthermore, The KDQOL-SFTM 1.3 includes general 36 items compensated with 43 kidney-disease specific items and an overall health assessment item for patients with chronic kidney disease (CKD). The KDQOL-SFTM assesses physical component summary score (PCS), mental component summary score (MCS), and kidney disease component summary score (KDCS) [7]. The Korean version of KDQOL-SFTM was recently translated and validated by Park et al [8]. Instruments and scoring programs of KDQOL-SFTM 1.3 can be found at http://www.gim.med.ucla.edu/kdqol/downloads/download.html.
In February 2008, demographic and laboratory findings were gained from the patients' self-reports and the medical record. Age, gender, marital status, religion, economic status, comorbidity (hypertension, diabetes mellitus, coronary artery disease, cerebrovascular disease, peripheral artery disease, malignancy), causes of ESRD, and duration of HD were reviewed. Hemoglobin (Hb), plasma glucose, serum albumin, blood urea nitrogen (BUN), and creatinine (Cr) were obtained from laboratory data at the entry point of this study. To quantify comorbidity, we utilized the modified Charlson comorbidity index (MCCI). The MCCI has been frequently used and validated in studies of HRQOL with ESRD patients [9].
From February 1, 2008 to February 28, 2011, we investigated enrolled patients' mortality, cardiovascular events, infection and complications that required hospitalization through the medical records, retrospectively. The cardiovascular events were defined as acute myocardial infarction, unstable angina requiring coronary intervention or bypass graft, and cardiac arrest. In addition, we analyzed the effect of depression and HRQOL on the patients' mortality and morbidity.
Statistical analysis
All analyses were performed using SPSS software (SPSS version 18.0.0). The results were given as mean±standard deviations (SD) for continuous variables and as proportions for categorical variables. Analyses included simple means and frequencies for baseline characteristics data, and unadjusted Cox's proportional hazard model was used to evaluate risk factors for mortality. All subjects were divided into two groups according to depression scores (BDI>18, BDI≤18), and into three groups according to tertiles of KDQOL-SFTM scores. The Kaplan–Meier method and the log rank test were used to assess and compare cumulative mortality rates between groups. The adjusted hazard ratios for all-cause mortality were calculated by Cox's proportional hazard model. Model 1 was adjusted for age, comorbidity score and serum albumin. Gender, duration of HD, Hb, glucose, marriage, religion and economic status were added in Model 2. Finally, we performed binary logistic regression analysis to determine the relationship between depression and morbidity (cardiovascular events, infection, and hospitalization) or tertiles of KDQOL-SFTM scores and morbidity. A P value of less than 0.05 was considered to be statistically significant. The study protocol was approved by the Institutional Review Board of Seoul National University Hospital. Informed consent was confirmed by the institutional review board (IRB).
Results
Baseline characteristics of patients
Table 1 shows the demographic, clinical and laboratory data. Of the 166 patients, the mean age was 57.9±14.0 years (range, 19–85 years). A total of 100 (60.2%) patients were male and 66 (39.8%) were female. A total of 136 (81.9%) patients were married, 112 (67.5%) had religion, and 98 (59.0%) were in middle economic status. The mean comorbidity score was 5.19±2.82 (range, 0–12) and 33.7% had diabetes mellitus. The most common cause of ESRD was diabetes mellitus (30.1%), followed by hypertension (19.3%) and glomerulonephritis (19.3%). The mean duration of HD was 6.2±5.7 years (range, 0.25–29 years), and 4.8% of the patients had undergone kidney transplantation previously. Additionally, the age of patients, comorbidity score and serum albumin level were significantly associated with mortality at a mean follow-up of 31.2 months (range, 1.5–36.9 months) by unadjusted Cox's proportional hazard model (P=0.021, 0.035 and 0.050, respectively).

Baseline Characteristics and Odds Ratios for Mortality
The mean BDI score was 14.25±9.89 in our patients. Among the 166 patients, 52 (31.3%) patients had depression when a BDI score of 18 was defined as a cut-off value, and 114 (68.7%) patients did not. Depression was significantly associated with old age (61.63±12.61 vs. 56.26±14.35 years, P=0.017) and low Hb level (10.12±0.97 vs. 10.74±1.24 g/dL, P=0.001), compared with patients without depression. However, male gender (51.9 vs. 64.0%, P=0.139), comorbidity score (5.6±2.8 vs. 5.0±2.8, P=0.188), diabetes (34.6% vs. 33.3%, P=0.871), mean duration of dialysis (5.6±5.8 vs. 6.5±5.7 years, P=0.378), and serum albumin level (3.93±0.34 vs. 4.00±0.37 g/dL, P=0.287) were not different statistically between two groups. Additionally, the mean PCS, MCS, and KDCS score were 54.9±21.6, 50.7±21.0, and 60.8±13.2 respectively. Decreased PCS was associated with old age, female gender, high comorbidity score, diabetes, and low albumin level (P<0.05). The factors associated with low MCS and KDCS score were old age and high comorbidity score (P<0.05).
During the mean 31.2 months follow-up period, 16 cases of death occurred. The causes of death were five myocardial infarction, two pericarditis, five infection including pneumonia and cholecystitis, one cancer, and three unknown causes. Cardiovascular event included myocardial infarction, unstable angina requiring coronary intervention or bypass graft, and cardiac arrest. Diabetes foot, pneumonia, tuberculous pericarditis, cholecystitis, paraspinal abscess, osteomyelitis, empyema, infected arteriovenous fistula, zoster, and influenza were included as infection events in this study. The complications that required hospitalization were infection, sepsis, myocardial infarction, unstable angina, complete atrioventricular block, stroke, gastric ulcer bleeding, ischemic colitis, pancreatitis, hepatic encephalopathy, dyspnea, electrolyte imbalance, and surgery for gastric cancer or bone fracture etc. The highest number of hospitalizations was up to five times. However, admission for percutaneous transluminal angioplasty for stenosis of arteriovenous fistula was excluded.
Influence of depression and HRQOL on all-cause mortality
The 3-year cumulative survival rate was 88.8%, and the depression did not affect the patients' survival (depression vs. nondepression: 91.8% vs. 87.2%, P=0.437 by log rank test) (Fig. 1). This trend remained consistent after multivariate adjustment by both Model 1 and Model 2. Univariate analysis showed that groups with upper tertiles in PCS were correlated with less mortality (OR, 0.12; 95% CI, 0.01 to 1.00; P=0.05) than lower tertiles (Fig. 2). In Cox's proportional hazards models by multivariate adjustment, there was some evidence of a trend that upper tertiles in PCS were correlated with less mortality ratios than lower tertiles, but this was not statistically significant. But, upper tertiles in MCS and KDCS were not correlated with higher survival rates than lower tertiles in both univariate and multivariate analysis (Table 2).
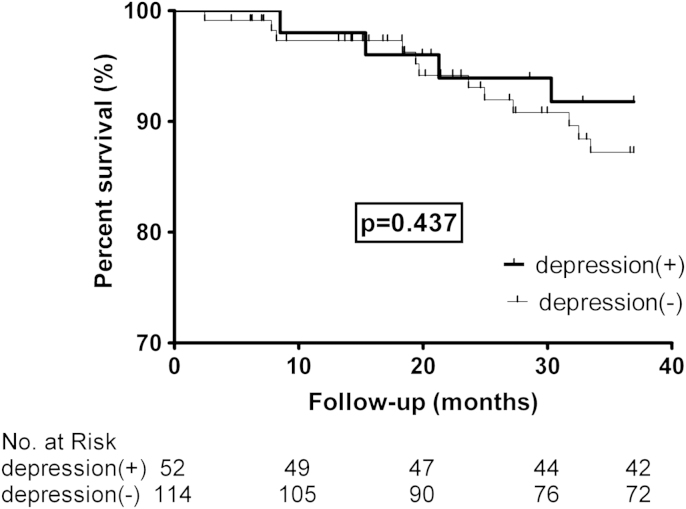
Kaplan–Meier survival curve according to depression. Cumulative survival estimation is assessed in patients according to depression which was evaluated by Beck's Depression Inventory (BDI) score. Patients with a BDI score of 18 or more were defined as a depression group.
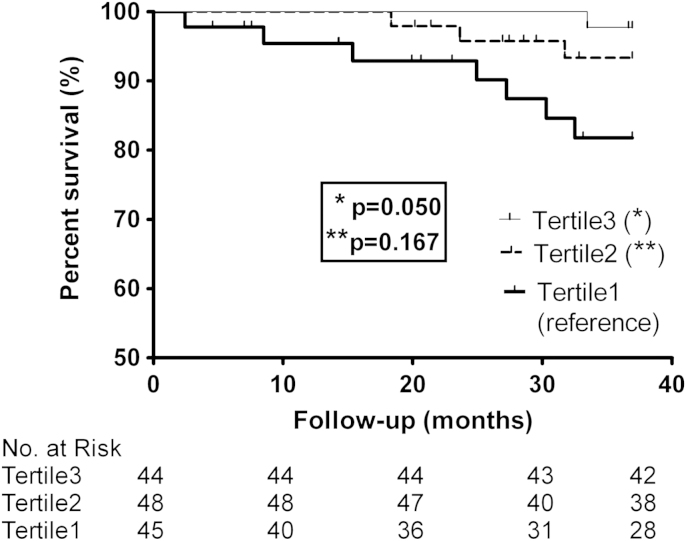
Kaplan–Meier survival curve according to physical component score (PCS). Cumulative survival estimation is assessed in patients according to the physical component score. Tertiles in physical component score: Tertile 1, <45.5; Tertile 2, 45.5–66.5; Tertile 3, >66.5.

Mortality Rate and Odds Ratios According to K-BDI and KDQOL-SF
Influence of depression and HRQOL on morbidity
The relationship of depression and HRQOL with enrolled patients' morbidity including cardiovascular events, infection, and complications that required hospitalization was evaluated. The depression did not affect any of the patients' morbidity among cardiovascular events, infection, and admission in both univariate and multivariate analysis (Table 3, Table 4, Table 5). But, upper tertiles in PCS were correlated with fewer cardiovascular events (OR, 0.09; 95% CI, 0.01 to 0.72; P=0.024) than lower tertiles. Even after adjusting for multiple variable including age, comorbidity index, and albumin, upper tertiles in PCS were correlated with fewer cardiovascular events than lower tertiles (OR, 0.08; 95% CI, 0.01 to 0.87; P=0.038). There was some evidence of a trend that upper tertiles in MCS and KDCS were correlated with fewer cardiovascular events than lower tertiles, but this was not statistically significant in both univariate and multivariate analysis (Table 3).

Cardiovascular Event Rate and Odds Ratios According to K-BDI and KDQOL-SF

Infection Rate and Odds Ratios According to K-BDI And KDQOL-SF

Admission Rate and Odds Ratios According to K-BDI and KDQOL-SF
The depression and any component summary score of KDQOL did not affect infection rate in our study in both univariate and multivariate analysis (Table 4). However, the upper tertiles and middle tertiles in KDCS were associated with less hospitalization than lower tertiles (OR, 0.38; 95% CI, 0.16 to 0.88; P=0.024 vs. OR, 0.39; 95% CI, 0.17 to 0.91; P=0.029, respectively) in unadjusted analysis. However, there were no statistical significance after adjusting for multivariate analysis in both Model 1 and 2. In addition, PCS and MCS were not correlated with admission rate in both univariate and multivariate analysis (Table 5).
Discussion
In the current study, we evaluated the effect of depression and HRQOL on patients' prognosis through mortality and morbidity among our maintenance HD patients. To our knowledge, this is the first report to reveal the effect of depression and HRQOL on HD patients' mortality and morbidity in Korea. Nephrologists have focused on not only traditional risk factors (e.g., diabetes mellitus, atherosclerosis and smoking), but also novel risk factors (e.g., epigenetic change, inflammation and oxidative stress) when evaluating mortality in CKD patients [10]. It is necessary to assess nontraditional risk factors, because an aging society encounters a wide variety of comorbidities. Depression is the most common psychological problem among ESRD patients [1], and has been shown to be related to mortality in patients hospitalized with medical illnesses [11] and myocardial infarction [12]. Also, HRQOL containing physical and mental health is realized to be an important predictive factor of mortality in ESRD patients [13]. However, clinicians have little concern for the importance of the role of depression and HRQOL.
In previous studies, the negative effect of depression, which was measured at commencement, on patients' survival has been often found. HD patients who showed less psychopathologic sign in initial investigations had improved prognosis [14]. And low depression score, young age, and high serum albumin level were related to better patient survival [15]. Likewise, some studies revealed that the BDI score and age were the significant predictive factors of mortality in ESRD patients [16]. However, previous studies usually did not fully control the confounding variables, such as comorbidity, nutrition, and dialytic interventional effects. In our analysis of maintenance HD patients, using a 31.2-month average follow-up period, we were unable to reveal the relationship of depression at baseline with patients' mortality and morbidity, when age, comorbidity score, and serum albumin concentration were adjusted as control variables. Similarly, other studies, which had relatively long-term follow-up periods, various psychosocial and medical information, and well-organized survival analyses, showed that depression at baseline was not associated with patients' mortality [17], [18], [19].
However, the time-varying analyses for impact of depression on mortality in HD patients demonstrated that the multiple measurement of depression was associated with mortality significantly in both univariate and multivariate analyses [2]. Multiple measurement of depression contributes a more realistic model than a single assessment of depression as a baseline value because time-varying covariate analyses yield unified and longitudinal evaluation of changes in depression over time. In addition, to analyze time-varying levels of depression at various points permits evaluating both fixed levels and dynamic changes in depression. Recently, depression is thought to be linked to malnutrition, inflammation or atherosclerosis in dialysis patients [20]. Thus, multiple measurement of depression could reflect dynamic changes of these factors better than a single assessment. Therefore, our results that whether the HD patients had depression or not was not significantly associated with patients' mortality in cross-sectional survey which evaluated only baseline level of depression were consistent with previous studies.
In the current study, 31.3% patients were found to have depression when a BDI score of 18 was defined as a cut-off value. Koo et al [21] suggested a BDI score of 21 as a cut-off value to define depression for Korean HD patients in their previous study. However, this result was based on small number of patients (n=62). On the contrary, a cut-off value of 16 for BDI score in elderly patients (age>60 years) was suggested by Jo et al [22] in their study of 2729 subjects in Korea. In order to avoid false-negatives, we considered it was reasonable to set 18 instead of 21 as a cut-off value, because the average age of our HD patients was 57.9 years. Moreover, we also analyzed the relationship between depression and mortality when 16 or 21 were defined as a cut-off value. Neither values affected the association between depression and patients' survival.
In the current study, PCS was correlated with mortality and cardiovascular events, and KDCS was associated with hospitalization. These results were consistent with previous reports. The importance of HRQOL in ESRD patients is well known. The study that measured the SF36 score in 1000 patients who underwent maintenance HD revealed that a low PCS was correlated with increased mortality and admission rates [23]. Another study of SF36 score in 65 ESRD patients found that HRQOL had a strong association with mortality and hospitalization [13]. Several hypotheses have been suggested to demonstrate the correlation between HRQOL and clinical prognosis. For instance, a discouraging self-evaluation of health status could activate a psychoneuroimmunologic reaction and interfere with taking health-protective behavior [24]. Some studies have shown that HRQOL was associated with nutritional factors, such as cholesterol, serum albumin, and hemoglobin levels and might conduct to poor clinical prognosis [13], [25]. But, the reason that subjective evaluation of health status after adjusting for chemical marker is associated with objective clinical outcome is not entirely interpreted.
Our study did not necessarily demonstrate a cause-and-effect relationship. Possibly, a medically worsening condition leads to a lower level of HRQOL and greater depressive affect in ESRD patients, subsequently resulting in death. The causality can only be identified in an analysis using interventional clinical trials. Many studies showed that nutritional markers including albumin, body mass index, and creatinine are strong predictive factors of HRQOL in ESRD patients [13], [26]. And depression could predict serum albumin concentration changes in ESRD patients in a study using a time-dependent approach [27]. Such data suggest possible mechanisms for mediating the deleterious effect of HRQOL and depression on patient prognosis. In other words, altered nutrition and immune system which were affected by HRQOL and depression could influence clinical outcome, as hypothesized in previous study [28]. Additionally, HRQOL and depression might be an indicator for unmeasured risk factors for mortality, for instance, maladaptive behaviors for unhealthy status [10], [11]. Further research is warranted to investigate the mechanisms that may be responsible for the relationship between HRQOL or depression and clinical outcome.
The current study has some limitations. First, the current study may be prone to selection bias, which is an inherent restriction of cohort studies. Because the patients in three university teaching hospitals and three local dialysis clinics in Seoul were included in this study, the population was confined to urban elderly Asian individuals. Therefore, our findings should be retested in HD programs in more varied ethnic and regional populations. Moreover, other selection bias is likely to be present because we excluded the patients who refused to enroll in this study or who were diagnosed with dementia. These patients might be more likely to have depression, lower HRQOL, and poor prognosis. Therefore, it is possible that our study could underestimate the influence of the depression and HRQOL on the prognosis. Second, we did not have information about cholesterol level, body mass index (BMI), and C-reactive protein that may serve as confounding factors. Third, HRQOL was also measured only once at the start of the present prospective study; therefore, our results do not show changes of HRQOL during the follow-up period. Fourth, interventions including psychological counseling and antidepressant medication during the study period were not evaluated in this study. The psychological intervention may influence the results. Finally, the relatively short-term follow-up period (mean 31.2 months), high survival rate (3-year cumulative survival rate: 88.8%) and small sample size (n=166) in this study may affect the result that depression was not a significant risk factor for mortality. Therefore, studies of long duration of follow-up and large number of patients should be needed. In the current study, data of total 35 patients were censored because of kidney transplantation (n=12), transfer to other hospitals (n=21), and follow-up loss of unknown cause (n=2). This censored data might affect the result of this study.
In conclusion, the cross-sectional survey of whether the HD patients had depression was not significantly associated with mortality and morbidity at a mean follow-up of 3 years. Among the each scale of KDQOL-SF, HRQOL was correlated with mortality, cardiovascular events, and hospitalization in univariate analysis. However, in multivariate analysis adjusted for other prognostic factors, only PCS was associated with cardiovascular event morbidity. Therefore, high-risk patients should be monitored more carefully and be invited to psychopharmacological therapy, and it might enhance patients' prognosis.
Conflict of interest
No conflict of interest.
References
Appendix A Supplementary data
Supplementary data
Acknowledgments
The authors would like to appreciate Jung Geon Lee at Namseoul Medical Clinic & Dialysis Unit, Seo Jin Yi at YSJ Internal Medicine Clinic and Eungtaek Kang at Kang Dialysis Clinic for collaboration in our survey.
Notes
Each author's specific contributions to the work are as follows. Hee Jung Jeon: research design, sample collection, data analysis, statistical analysis, writing of the paper. Hayne Cho Park, Ji In Park: research design, data collection. Jung Pyo Lee, Kook-Hwan Oh, Ho Jun Chin, Kwon Wook Joo: sample collection, data analysis. Yon Su Kim, Chun Soo Lim, Curie Ahn, Jin Suk Han, Suhnggwon Kim: data analysis, statistical analysis. Yun Kyu Oh: research design, sample collection, data analysis, writing of the paper.
All authors have never submitted the manuscript, in whole or in part, to other journals.
Supplementary data associated with this article can be found in the online version at doi:10.1016/j.krcp.2012.01.001.