Advances in the management of diabetic kidney disease: beyond sodium-glucose co-transporter 2 inhibitors
Article information

Abstract
Progress in the treatment of diabetic kidney disease (DKD) has been modest since the early trials on renin-angiotensin-aldosterone system inhibitors (RAASis). Although sodium-glucose co-transporter 2 inhibitors (SGLT2is) have revolutionized the management of DKD by lowering proteinuria and protecting organs, other novel treatment approaches with good evidence and efficacy that can be used in conjunction with a RAASi or SGLT2i in managing DKD have emerged in the past few years. This review discusses the evidence for glucagon-like peptide-1 receptor agonist, selective mineralocorticoid receptor antagonist, and selective endothelin A receptor antagonist, emerging treatment options for DKD beyond SGLT2 inhibition.
Introduction
Diabetes is a global health issue, and the prevalence of its complications has increased in the past few decades. Approximately one in 11 people in the world suffers from diabetes, and 87% to 90% of those patients have type 2 diabetes mellitus (T2DM) [1]. Diabetic kidney disease (DKD) is the leading cause of chronic kidney disease (CKD). Approximately 40% of T2DM patients develop DKD, and about 10% of deaths from T2DM are due to kidney failure [2]. The Asian population is more vulnerable to DKD than people in Western countries [3]. A genetic component could be involved because DKD causes more end-stage kidney disease among the Asian population in China, the USA, and Eastern Europe than it does in people of other ethnicities.
Different pathways have been found in the pathophysiology of DKD. Metabolic factors such as hyperglycemia and hyperalbuminuria can alter hemodynamics by increasing local angiotensin production, which leads to afferent arteriole dilatation and efferent arteriole constriction. The consequent glomerular hyperfiltration or increase in intraglomerular pressure can cause chronic kidney damage. Those metabolic factors also promote interstitial inflammation, which leads to extracellular matrix (ECM) accumulation, interstitial fibrosis, and irreversible kidney damage [2,4].
Sodium-glucose co-transporter 2 inhibitors (SGLT2is) have their effects at the proximal convoluted tubule, where they increase glucose reabsorption, urinary glucose excretion, and natriuresis [5,6]. The unique mechanism of SGLT2is causes pleiotropic effects that reduce hyperglycemia, hemoglobin A1c (HbA1c), weight, and blood pressure [7–10]. Several studies have focused on the renal-specific outcomes of SGLT2is and found that they have renoprotective effects, largely due to their ability to reduce sodium reabsorption at the proximal tubule, which improves intraglomerular pressure and reduces hyper-perfusion [11,12]. Cardiovascular death was also reduced in CKD patients who used an SGLT2i [13]. Although SGLT2is and renin-angiotensin-aldosterone system inhibitors (RAASis) are widely combined in the nephrology community, initiation of that practice is not recommended in patients with an estimated glomerular filtration rate (eGFR) of <30 mL/min/1.73 m2, and it should be discontinued when patients require kidney replacement therapy [14].
During the past few years, more treatment options have been investigated in conjunction with RAASi and SGLT2i treatment to slow the progression of DKD (Tables 1, 2). This review revisits conventional management strategies for DKD: lifestyle modifications, glycemic and blood pressure control, and RAASi use. The mechanisms and preclinical and major clinical studies for new treatments, specifically glucagon-like peptide-1 receptor agonists (GLP-1 RAs), nonsteroidal mineralocorticoid receptor antagonists (MRAs), and selective endothelin A receptor antagonists (ERAs) are then reviewed.

Novel therapeutic agents for diabetic kidney disease

Summary of currently available GLP-1 RAs, selective MRAs, and selective ERAs, with dosages
Lifestyle modification
Lifestyle modifications, such as exercise, smoking cessation, and diet control, are the backbone of DKD management. The DASH (Dietary Approaches to Stop Hypertension) diet, which is high in vegetables, fruit, and low-fat dairy products, improved systolic blood pressure and 24-hour blood pressure measurements in primary hypertension patients [15]. The guideline for diabetes patients with CKD published in 2020 by Kidney Disease Improving Global Outcomes (KDIGO) recommends an individualized dietary prescription made using shared decision making. A balanced healthy diet of high-fiber foods (vegetables and fruit), plant-based protein, legumes, and unsaturated fat is encouraged. The guideline recommends protein intake of 0.8 g/kg of body weight/day for DKD patients who are not on renal replacement therapy and 1 to 1.2 g/kg of body weight/day in patients treated with hemodialysis or peritoneal dialysis. Processed meat, refined carbohydrates, and sweetened beverages are not recommended. Sodium should be restricted to <2 g/day to reduce the risk of CKD progression and increased blood pressure. A regular exercise regime, with at least 150 minutes of moderate-intensity exercise per week, has also been recommended for patients with DKD [16]. Obese patients are recommended to undertake a structured program of weight reduction. Metformin, SGLT2is, and GLP-1 RAs could have additional benefits in weight loss [17]. However, clinicians are advised to be cautious with caloric restriction, especially in patients with advanced CKD, because it can lead to malnutrition and other adverse outcomes [16].
Glycemic control
In various clinical studies, tight glycemic control has shown benefits in reducing diabetes-related microvascular complications. The UKPDS (UK Prospective Diabetes Study) group compared patients with tight glycemic control, with an average HbA1c of 7.4%, with a control group with an HbA1c of 8%. A 32% reduction in diabetes-related endpoints and a 36% reduction in all-cause mortality during follow-up were seen in the tight control group [18], and the microvascular risk reduction persisted for 10 years, as shown by a follow-up study [19]. In the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation) trial, the intensive treatment arm, in which HbA1c was kept <6.5%, demonstrated a 21% reduction in diabetic nephropathy and albuminuria compared with the conventional group [20]. In a post-study analysis of ADVANCE data, a reduction in end-stage kidney disease was the only positive finding with statistical significance in the intensive treatment group (hazard ratio [HR], 0.54; p = 0.007), and no benefit was found in preventing renal-disease-related deaths [21]. Furthermore, in the Veterans Affairs Diabetes Trial, intensive diabetes control to an average HbA1c of 6.9% showed no significant benefit in microvascular complications [22].
The current KDIGO guideline recommends an individualized HbA1c target ranging from 6.5% to 8%, depending on the risk profile for developing hypoglycemia, whereas the Asian Pacific Society of Nephrology (APSN) guideline suggests that the target not be lower than 7% to balance the risks of micro- and macrovascular complications against the development of hypoglycemia [17]. The glycemic target should definitely be individualized based on the patient’s severity of CKD, life expectancy, comorbidities, macrovascular complications, propensity of treatment to hypoglycemia, and awareness.
Blood pressure control
Intensive and individualized blood pressure control is recommended not only for the management of T2DM [23], but also in DKD to prevent cardiovascular mortality, the progression of kidney disease, and albuminuria. In the ACCORD (Action to Control Cardiovascular Risk in Diabetes) blood pressure trial, 4,733 patients with T2DM were randomized to receive intensive therapy (systolic blood pressure target of <120 mmHg) or standard therapy (systolic blood pressure of <140 mmHg). After a mean follow-up of 4.7 years, the incidence of macroalbuminuria was lower in the intensive treatment arm, but the incidence of microalbuminuria did not differ significantly [24]. A systematic review of three other randomized controlled trials also concluded that lowering the blood pressure target had benefits for patients with macroalbuminuria [25]. Similar findings were reported for Asian DKD patients with heavy proteinuria (urine protein to creatinine ratio, >1 g/gCr); a target systolic blood pressure of ≤ 130 mmHg offered renoprotection and cardioprotection [26].
The current APSN clinical guideline for DKD recommends that blood pressure be lowered toward 130/80 mmHg to offer stroke and cardiovascular protection and slow kidney disease progression [17]. In the 2021 Joint Association of British Clinical Diabetologists and UK Kidney Association guideline, the blood pressure target varies with the stage of CKD and degree of proteinuria. For patients with T2DM and a urine albumin to creatinine ratio (UACR) of <3 mg/mmol, the target blood pressure should be less than 140/90 mmHg. For patients with a UACR > 3 mg/mmol, the target blood pressure should be less than 130/80 mmHg. However, caution should be used if blood pressure is not measured in a standardized manner, and a less aggressive approach should be offered to patients with a short life expectancy [27].
Renin-angiotensin-aldosterone inhibition
RAASis—angiotensin converting enzyme inhibitors (ACEis) and angiotensin II receptor blockers (ARBs)—are widely used in hypertension management. Their ability to reduce proteinuria is predominantly due to their effect on the vasodilation of the glomerulus efferent arterioles, as has been shown in various clinical trials. In the Irbesartan Diabetic Nephropathy trial, 1,715 patients with DKD were randomized to receive irbesartan, amlodipine, or placebo. The patients who received irbesartan had a lower incidence of doubling serum creatinine and slower progression to end-stage kidney disease or kidney-related death than those in the amlodipine (23% reduction) and placebo (20% reduction) groups [28]. In the RENAAL (Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan) trial, 1,513 DKD patients were randomized to receive 50 mg or 100 mg of losartan daily, in addition to their conventional antihypertensive treatment. A 20% of reduction in end-stage kidney disease or renal-related death was observed. Proteinuria and the incidence of first admission of heart failure were also reduced compared with the placebo group [28–30]. A similar result was seen in the Randomized Olmesartan and Diabetes Microalbuminuria Prevention trial: patients who received olmesartan had a lower incidence of microalbuminuria than those in the placebo group. The treatment group also had a delayed onset of microalbuminuria (23% slower than the placebo group). However, major cardiovascular events were more frequent in the olmesartan arm, especially among patients with preexisting ischemic heart disease [31].
Hyperkalemia, hypotension, and acute kidney injury were the most frequent adverse events noted in those studies. Moreover, based on the results of the Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint trial, combining an ACEi and ARB is not recommended. Patients on both an ACEi and ARB did not have any additional benefit in terms of proteinuria reduction, but they did have an increased risk of adverse events [29]. To prevent adverse events, blood pressure, serum creatinine, and potassium should be monitored within 2 to 4 weeks of starting or adjusting the dosage of an ACEi or ARB. An acute (30%) rise in serum creatinine level from baseline within 4 weeks of initiating treatment or increasing the dose should lead clinicians to rule out any underlying cause, such as hypovolemia, concomitant medications, or renal artery stenosis. In addition, dietary potassium restriction should be reenforced, and concurrent drugs (e.g., an aldosterone antagonist) that can lead to hyperkalemia should be reviewed. Adding diuretics or sodium bicarbonate can ameliorate hyperkalemia [16].
Glucagon-like peptide-1 receptor agonist
GLP-1 is an incretin hormone from intestinal cells that is secreted in response to food intake. It acts with an independent pathway from insulin to lower the blood glucose level and achieve postprandial glucose homeostasis. In humans, GLP-1 receptors are found predominantly in glomerular and proximal tubular cells; the natriuretic and diuretic properties of GLP-1 can influence renal hemodynamics [32]. Moreover, the kidneys are the major site of excretion of GLP-1, glucose-dependent insulinotropic peptide (GIP), and their metabolites. Although GLP-1 and GIP levels increase in patients with renal failure, those inactive forms of incretin hormones do not have any renoprotective effects on patients [33].
In animal models, GLP-1 agonist has shown renoprotective effects by reducing inflammation and promoting antifibrosis in the renal parenchyma. Those effects are independent of its ability to lower blood glucose. Exendin-4 promotes ABCA1 expression in glomerular endothelial cells and decreases renal cholesterol accumulation, which alleviated inflammation and proteinuria in diabetic mice [34]. An injection of liraglutide into spontaneously diabetic Torii fatty rats produced food intake, weight, blood pressure, and blood glucose reductions, downregulated the renal expression of p-mTOR, and increased the expression of LC3B-II, a marker of autophagy [35]. Another study demonstrated that giving low-dose lixisenatide to early-onset diabetic rats reduced renal transforming growth factor-β1 (TGF-β1) and exhibited antioxidant effects, such as increased iNOS and COX-2 production [36]. In rat mesangial cells treated with advanced glycation end products (AGEs), a GLP-1 receptor agonist had an anti-inflammatory effect by attenuating the production of AGE-induced interleukin-6, tumor necrosis factor-α, and AGE receptors [37].
GLP-1 RA treatment reduced ECM production via different pathways (Fig. 1). For example, a GLP-1 RA reduced fibronectin and collagen IV production by glomerular mesangial cells [38]. It also inhibited the proliferation of human mesangial cells, which upregulate TGF-β1 and connective tissue growth factor, thereby reducing ECM production and preventing fibrosis in the glomerular mesangium [39]. In a streptozotocin-induced type 1 diabetes mouse model, liraglutide attenuated Wnt/β-catenin signaling proteins and reduced glomerular fibronectin, collagen type IV, and α-smooth muscle actin, which reduced glomerular ECM accumulation and renal injury [40].
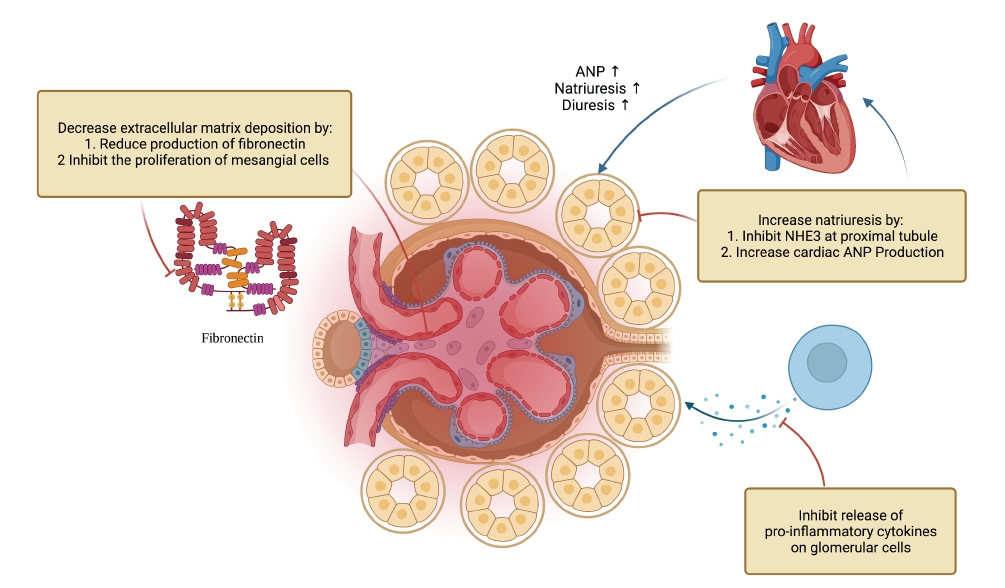
The biological mechanism of GLP-1 receptor agonist.
ANP, atrial natriuretic peptide; GLP-1, glucagon-like peptide-1; NHE3, Na+/H+ exchanger 3.
A GLP-1 RA showed an immunomodulatory effect that prevented macrophage and T cell infiltration and reduced intercellular adhesion molecule-1 (ICAM-1) and type IV collagen accumulation. GLP-1 RA cleavage products also exhibited immunomodulatory effects that attenuated the renal accumulation of macrophages and T cells [41]. GLP-1 RAs can also act on GLP-1 receptors on macrophages, monocytes, or glomerular endothelial cells to inhibit the release of pro-inflammatory cytokines from macrophages and ICAM-1 on glomerular cells [42]. A similar effect was seen in a murine model of nephrotoxic serum nephritis: a GLP-1 RA blocked the glycolysis of T cells, which decreased Glut1 messenger RNA (mRNA) expression and the proliferation of TH1 and TH17 cells [43].
The diuresis and natriuresis effects of GLP-1 RAs were seen in both experimental and human studies and occurred via renal and extra-renal mechanisms. GLP1-RAs target Na+/H+ exchanger 3 (NHE3), which is found at the proximal tubule. NHE3 was found to reabsorb filtered sodium from the glomerulus and increase the glomerular pressure through tubuloglomerular feedback, similar to that seen with the sodium-glucose co-transporter. The GLP-1 RA was observed to inactivate or induce the phosphorylation of NHE3, which increased natriuresis [44]. The extra-renal natriuresis effects of GLP-1, including cardiac and neuronal responses to GLP-1, have also been studied. Liraglutide was found to activate GLP-1 receptors at cardiac myocytes, which increased the secretion of atrial natriuretic peptide and promoted natriuresis [45].
Several early clinical studies examined the renoprotective effect of combining a GLP-1 RA with oral antidiabetic agents or insulin (Table 3). A small study that combined weekly liraglutide with a RAASi reduced albuminuria by 32% and average systolic blood pressure by 5 mmHg [46]. In a post hoc comparison of data from patients using once-weekly exenatide and those using a non-GLP-1 receptor agonist (both groups received the maximum tolerated dose of a RAASi), a 26.2% reduction in albuminuria was seen, and its effect was independent of baseline RAASi usage [47,48]. In a post hoc analysis for the data of DECREASE (Dapagliflozin Plus Exenatide on Central REgulation of Appetite in diabeteS typE 2) study, the combination of twice-daily exenatide and dapagliflozin was found to have a synergistic effect in reducing mean urine albuminuria compared with the use of dapagliflozin alone; –39.6% vs. –18.1% in UACR compared with baseline [49]. Another study compared exenatide plus glargine to lispro plus glargine and showed a greater UACR change in the exenatide group. Weight loss was observed in the exenatide group (–1.38 ± 0.63 kg), and weight gain was seen in the insulin group (+1.30 ± 0.66 kg) [50]. In future therapeutic use, GLP-1 RAs might work in conjunction with mesenchymal stem cells to stabilize inflammation and fibrosis while the mesenchymal stem cells restructure the renal parenchyma [51].

Summary of clinical trials of GLP-1 RAs and renal outcomes
In large-scale human clinical studies, GLP-1 RAs showed positive effects in slowing the progression of DKD, though the early data were mainly from cardiovascular or diabetes studies. In the LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) trial, 9,340 patients with T2DM were recruited to receive liraglutide or placebo, and patients’ cardiovascular outcomes were investigated. DKD events were lower in the liraglutide arm than in the placebo arm (1.5 vs. 1.9 events per 100 patient-years of observation), and CKD progression was slowed in patients with eGFR of <30 mL/min/1.73 m2 [52,53]. A similar effect was demonstrated in the SUSTAIN-6 (Trial to Evaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Subjects with Type 2 Diabetes) study: patients with established cardiovascular disease or associated risk factors were treated with semaglutide (0.5 mg or 1 mg once a week) or placebo. The rate of new-onset DKD was lower in the semaglutide arms (3.8% vs. 6.1%; HR, 0.64; 95% confidence interval [CI], 0.46–0.88) [54]. In the AMPLITUDE-O (Effect of Efpeglenatide on Cardiovascular Outcomes) study, efpeglenatide, a long-acting GLP-1 RA that has a structure similar to human GLP-1, reduced the renal composite outcome (decrease in eGFR of >40% for >30 days or end-stage kidney disease) by 32% [55]. In an exploratory analysis of the ELIXA (Evaluation of Lixisenatide in Acute Coronary Syndrome) study that specifically targeted renal outcomes, lixisenatide was found to reduce proteinuria in patients with different preexisting severities of proteinuria, and eGFR did not change significantly [56]. In an exploratory analysis of the REWIND (Researching Cardiovascular Events with Weekly Incretin in Diabetes) study, dulaglutides reduced the incidence of first-onset microalbuminuria in T2DM patients (HR, 0.77; 95% CI, 0.68–0.87; p < 0.0001), the rate of decline in eGFR, and the incidence of chronic renal replacement therapy initiation [57].
The AWARD-7 (Dulaglutide versus insulin glargine in patients with type 2 diabetes and CKD) study examined the renal outcomes of patients with moderate to severe DKD and demonstrated that GLP-1 RAs have a unique class effect. AWARD-7 included 576 patients with stage 3–4 DKD who all received maximum RAASi therapy, oral hypoglycemic agents, and/or insulin before randomization. Patients were randomized to receive weekly dulaglutide (0.75 mg or 1.5 mg) or glargine insulin for 52 weeks, and changes in HbA1c and UACR and the rate of decline in eGFR were examined. The study found no significant change in UACR compared with baseline, but the rate of eGFR decline was slower in the dulaglutide groups (–1.1 mL/min/1.73 m2 and –1.5 mL/min/1.73 m2 with 1.5 mg and 0.75 mg, respectively), and the incidence of end-stage kidney disease was also lower in the dulaglutide groups [58]. Compared with other cardiovascular event-orientated studies in which the treatment of T2DM and hypertension varied among patients, the AWARD-7 study successfully demonstrated an independent class effect for renoprotection, which can be related to the mechanism discussed.
In terms of adverse events, lixisenatide had a higher incidence of gastrointestinal adverse events than placebo (by 14%) [59]. Several cases of acute kidney injury were associated with GLP-1 RA treatment, mainly acute tubular injury [60]. Liraglutide is recommended over exenatide because exenatide is predominantly excreted via renal mechanisms, but caution should be exercised with liraglutide because it lacks adequate pharmacokinetic data [61]. None of the major clinical studies discussed above reported any significant adverse events.
In summary, GLP-1 RAs have been shown to improve weight loss, hypertension, glycemic control, and UACR. The renoprotective effect was attributed to their ability to target immunomodulatory pathways, reduce the release of inflammatory cytokines, downregulate the chemoattraction of inflammatory cells, and reduce intracellular matrix deposition and subsequent interstitial fibrosis. They also increase natriuresis and diuresis, which can alter renal hemodynamics. Both RAASis and SGLT2is target glomerular hemodynamics by altering renal perfusion or tubuloglomerular feedback, but they do not alter renal interstitial inflammation. The additional natriuresis and anti-inflammatory effects of GLP-1 RAs can be another tool for managing advanced CKD. Most of the clinical evidence discussed is based on post hoc analyses of data from cardiovascular trials. The AWARD-7 study demonstrated that GLP-1 RAs have a potential class effect independent of blood pressure and glycemic control. More renal outcome-orientated studies of different GLP-1 RAs should be conducted to strengthen the evidence for that unique class effect.
Nonsteroidal selective mineralocorticoid receptor antagonist
Aldosterone has multiple extra-renal effects, including the induction of inflammation, increased vascular rigidity, collagen formation, and the stimulation of fibrosis. Blocking the mineralocorticoid receptor can prevent or slow the progression of heart or kidney disease [62]. Steroidal MRAs, e.g., spironolactone or eplerenone, can prolong survival in cardiac failure patients by improving hypertension and having antifibrosis and anti-inflammatory effects [63,64]. However, it is underused in CKD, even though it has been shown to improve proteinuria, because it carries a risk of hyperkalemia, as shown in a previous meta-analysis [65].
Finerenone (Fig. 2), a nonsteroidal selective MRA, was found in animal studies to have renoprotective effects and ameliorate proteinuria with few adverse events [66]. Rodent models of T1DM and T2DM show an increase in the expression of mineralocorticoid receptors at the protein and mRNA levels, apart from albuminuria and renal injury. Other factors that contribute to the activation of inflammatory cells such as TGF-β mRNA and osteopontin mRNA were also increased in those models. Those factors were downregulated with the use of an MRA, which indicates that MRAs might have a role in reducing inflammation and fibrosis [67].
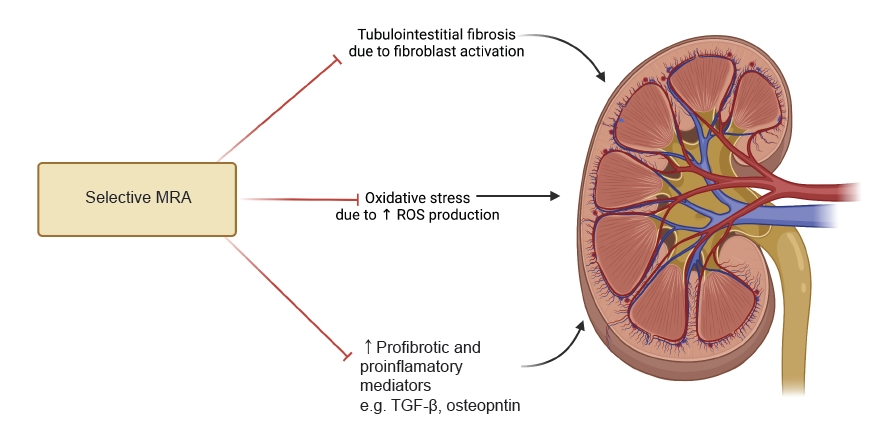
The biomechanism of selective mineralocorticoid receptor antagonist.
MRA, mineralocorticoid receptor antagonist; ROS, reactive oxygen species; TGF-β, transforming growth factor-β.
Selective MRAs also show antifibrosis effects in animal cardiac models. For example, in a preclinical model with deoxycorticosterone acetate and salt-challenged rats, finerenone not only prevented kidney damage and proteinuria but also reduced cardiac damage and ventricular hypertrophy [68]. In phase 2 clinical studies, finerenone was found to ameliorate UACR after 90 days of treatment in DKD patients [69,70]. Other agents, such as apararenone (phase II study) and esaxerenone (phase III study), were shown to reduce proteinuria (Table 4) [71,72].

Summary of clinical trials of nonsteroidal mineralocorticoid receptor antagonists and renal outcomes
The FIDELIO-DKD (Finerenone in Reducing Kidney Failure and Disease Progression in Diabetic Kidney Disease) study is a major human clinical study on finerenone in which 5,734 patients with DKD stage 3b to 4 were randomized to receive finerenone or placebo with the maximum tolerated dose of a RAASi. In a median follow-up of 2.6 years, the finerenone group had fewer renal composite events (kidney failure, sustained decrease in eGFR of at least 40% from baseline, or death from renal causes) than the placebo group [73]. A subsequent study also demonstrated that finerenone treatment reduced composite kidney outcomes in patients with a history of cardiovascular disease (15.3% in finerenone group vs. 20.5% in placebo group) [74]. However, in a post hoc safety analysis, hyperkalemia was more common in the finerenone arm (21.4% with serum potassium level of >5.5 mmol/L and 4.5% with >6 mmol/L) [75].
The FIGARO-DKD (Finerenone in Reducing Cardiovascular Mortality and Morbidity in Diabetic Kidney Disease) study tested finerenone in patients with less severe CKD than those in the FIDELIO-DKD study, and its focus was on the cardiovascular outcome. Finerenone reduced the incidence of death from cardiovascular causes compared with placebo (12.4% vs. 14.2%). Kidney failure and death from renal causes were also less common in the finerenone arm (9.5% vs. 10.8%) [76].
Overall, finerenone has renoprotective effects, and evidence shows that it reduces proteinuria, likely as a result of its anti-inflammatory and antifibrotic effects. Despite a higher incidence of hyperkalemia in the finerenone arm of the FIDELIO-DKD study, the discontinuation rate was lower than in other clinical studies that combined a RAASi with a specific target and intervention for hyperkalemia during the study period [77,78]. The patients in the FIDELIO-DKD study had relatively advanced CKD, so regardless of the study result and rate of adverse events, dietary restriction of potassium and careful monitoring during treatment would be highly recommended for such patients.
Selective endothelin A receptor antagonist
Endothelin-1 (ET-1) can be stimulated by different factors in DKD, such as an increase in the insulin level, hyperglycemia, or acidemia [79]. It has multiple pathological effects, including the alteration of renal blood flow and glomerular filtration by the activation of ETA receptors in the vascular smooth muscles of the glomeruli and small vessels of the kidney. ET-1 can also cause renal inflammation by increasing the production of inflammatory cytokines and growth factors, and it promotes the chemoattraction of macrophages in the kidney and subsequently increases interstitial matrix deposition.
ERAs have been available since the early 1990s and have been used mainly to treat hypertension through their reduction of renal vascular tone (Fig. 3). Moreover, ERAs ameliorate renal interstitial inflammation and fibrosis. An early preclinical study showed that a selective ERA reduced the progression of DKD by improving vascular tone, decreasing the production of inflammatory cytokines (including TGF-β), and attenuating macrophage infiltration [80].
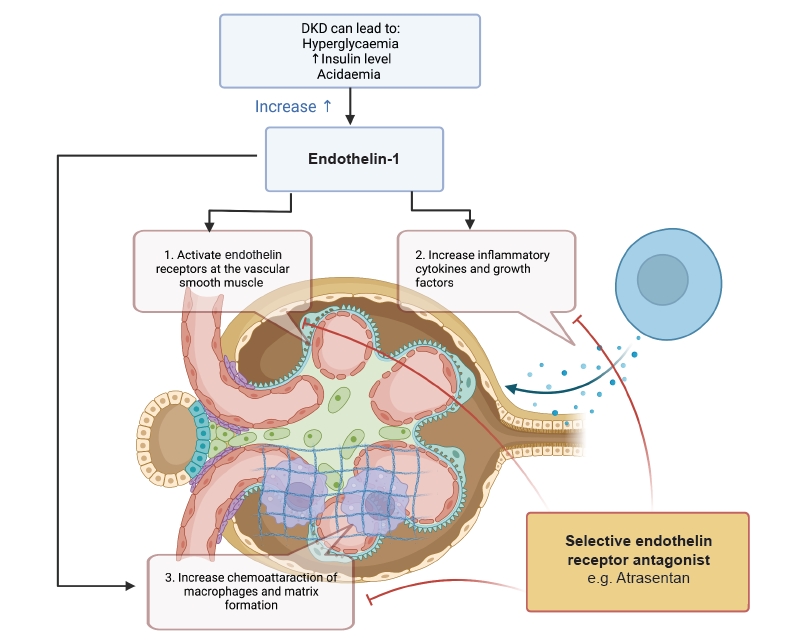
The biomechanism of selective endothelin receptor antagonist.
DKD, diabetic kidney disease.
A human clinical study showed that an ERA improved blood pressure and the systemic vascular index [81]. Clinical studies of avosentan demonstrated improvement in UACR and dyslipidemia in DKD patients [82,83]. In those studies, fluid overload and exacerbation of cardiac failure were the most common adverse effects [84–87]. A human clinical study of atrasentan showed that it had a renoprotective effect when it was used in conjunction with a RAASi. In that study, 51% of the DKD patients who received 0.75 mg of atrasentan and 55% of the patients who received 1.25 mg of atrasentan had proteinuria reductions compared with the placebo group. Improvements in low-density lipoprotein cholesterol, triglycerides, and 24-hour blood pressure monitoring were also reported in that study. However, the dropout rate was relatively high among patients receiving the higher dose of atrasentan due to intolerance of weight gain and anemia [88].
A similar study was stopped early due to a high number of similar adverse events.
The SONAR (Study of Diabetic Nephropathy with Atrasentan) is the largest randomized controlled trial to date to investigate the efficacy of ERA. Patients had to enter a 6-week “enrichment period” in which they received 0.75 mg of atrasentan daily to monitor them for any adverse events before they were randomized for the main trial. In the main trial, 4,711 patients with stage 2 to 4 DKD and a UACR between 300 and 5,000 g/mg were randomized to continue taking atrasentan or receive placebo. A 35% to 38% reduction in proteinuria was seen in the atrasentan arm. Both studies concluded that fluid retention and exacerbation of heart failure were common side effects, but the incidence of those effects did not differ significantly from placebo [89]. A post hoc analysis of the SONAR data that compared pretrial eGFR to eGFR during the trial period found a reduction in the rate of eGFR decline in the atrasentan group compared with the placebo group [90].
Early clinical studies of ERAs demonstrated positive results for renal outcomes, such as a reduction in albuminuria (Table 5 [81–83, 88–90]). However, a high rate of adverse events such as fluid overload, the exacerbation of cardiac failure, and death, outweighed those therapeutic effects, which might explain the lack of further clinical studies of ERAs. The SONAR study heralded the positive potential of ERA for managing DKD, but it seems to be suitable only for a highly selected group and requires careful clinical monitoring. Moreover, clinicians should be cautious about the adverse effects of ERAs, primarily fluid overload and the exacerbation of cardiac failure. A trial period of ERA use with close monitoring for adverse reactions could be useful. Overall, more clinical studies with different ERAs should be conducted to clarify their efficacy and adverse effects.

Clinical trials of selective endothelin A receptor antagonists in DKD
Conclusion
For the past 20 years, RAASis have been the only treatment with evidence to show that they reduce proteinuria and the progression of kidney disease. The advent of SGLT2is thus changed the landscape of DKD management. Despite their effectiveness, the current guidelines do not recommend that an SGLT2i be initiated in patients with an eGFR < 30 mL/min/1.73 m2, and SGLT2i treatment should be stopped when a patient requires kidney replacement therapy. GLP-1 RA treatment does not require a dose adjustment according to eGFR, so it could potentially fill that treatment gap [16]. Finerenone and atrasentan might offer additional benefits when used with conventional therapy. However, more real-world data are required to demonstrate their efficacy and safety. Despite those advances, lifestyle modifications and regular DKD complication screening using the UACR in diabetes patients should be emphasized in the primary care setting to avoid missing the window of opportunity for initiating specific treatments.
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.
Funding
ATPC was supported by the Croucher Senior Medical Fellowship, which was awarded to SCWT in 2019. This work is also supported by philanthropic donations from the Mr & Mrs Tam Wing Fan Edmund Renal Research Fund, Dr. Rita T Liu SBS of the L & T Charitable Foundation Ltd. & the Bingei Family of Indo Café, Mr. Winston Leung, Mr. K.K Chan of Hong Kong Concrete Co. Ltd., Ms. Lau Siu Suet, and an Endowment Fund established at the University of Hong Kong for the “Yu Professorship in Nephrology” awarded to SCWT. The funding bodies had no role in writing the manuscript.
Authors’ contributions
Writing–original draft: ATPC
Writing–review & editing: ATPC, SCWT
All authors read and approved the final manuscript.