Risk of ventricular tachycardia and its outcomes in patients undergoing continuous renal replacement therapy due to acute kidney injury
Article information

Abstract
Background
Despite efforts to treat critically ill patients who require continuous renal replacement therapy (CRRT) due to acute kidney injury (AKI), their mortality risk remains high. This condition may be attributable to complications of CRRT, such as arrhythmias. Here, we addressed the occurrence of ventricular tachycardia (VT) during CRRT and its relationship with patient outcomes.
Methods
This study retrospectively enrolled 2,397 patients who started CRRT due to AKI from 2010 to 2020 at Seoul National University Hospital in Korea. The occurrence of VT was evaluated from the initiation of CRRT until weaning from CRRT. The odds ratios (ORs) of mortality outcomes were measured using logistic regression models after adjustment for multiple variables.
Results
VT occurred in 150 patients (6.3%) after starting CRRT. Among them, 95 cases were defined as sustained VT (i.e., lasting ≥30 seconds), and the other 55 cases were defined as non-sustained VT (i.e., lasting <30 seconds). The occurrence of sustained VT was associated with a higher mortality rate than a nonoccurrence (OR, 2.04 and 95% confidence interval [CI], 1.23–3.39 for the 30-day mortality; OR, 4.06 and 95% CI, 2.04–8.08 for the 90-day mortality). The mortality risk did not differ between patients with non-sustained VT and nonoccurrence. A history of myocardial infarction, vasopressor use, and certain trends of blood laboratory findings (such as acidosis and hyperkalemia) were associated with the subsequent risk of sustained VT.
Conclusion
Sustained VT occurrence after starting CRRT is associated with increased patient mortality. The monitoring of electrolytes and acid-base status during CRRT is essential because of its relationship with the risk of VT.

Introduction
Acute kidney injury (AKI) is a common complication in critically ill patients, and interest in this condition has increased due to its relationship with high mortality [1,2]. Continuous renal replacement therapy (CRRT) is frequently the first option used to treat patients with severe AKI who require renal replacement therapy, particularly when they are hemodynamically unstable [3–5]. Despite the success of the therapeutic approach with this modality, the mortality rates have not decreased to <50% over the past two decades [2,6,7]. Several adverse events that may arise in patients on CRRT may hinder its clinical usefulness, even with appropriate initiation [8–10]; these adverse events include hypotension, an imbalance in major and minor electrolytes, hypothermia, hematologic abnormalities, and catheter-related complications [9]. Certain arrhythmias may occur during CRRT [6,9,11]; new-onset atrial fibrillation has been reported in >10% of patients on CRRT, and its occurrence is associated with worse patient outcomes [11]. Other arrhythmias may also occur, but their characteristics, risk factors for occurrence, and subsequent outcomes have not been thoroughly evaluated.
Ventricular tachycardia (VT) is a rare subset of arrhythmias in healthy individuals, but it may frequently occur if abnormalities in the heart structure, metabolites, and electrolytes exist [12]. Patients undergoing hemodialysis may be at extremely high risk of VT because they have myocardial fibrosis, a microvascular disorder, left ventricular hypertrophy, and electrical instability due to the repeated fluid shifts that occur during hemodialysis [13]. Similarly, patients with CRRT typically experience regional impairment in cardiac contractility [14]; thus, VT may occur in patients on CRRT, but no studies have examined this issue. The present study evaluated the prevalence of VT in patients after starting CRRT due to AKI, predictors related to its occurrence, and its relationship with overall mortality outcomes.
Methods
Patients and data collection
This was a retrospective observational study of 2,832 patients who underwent CRRT at Seoul National University Hospital from June 2010 to December 2020. Among these, patients who were under 18 years old (n = 58) and those who had been on chronic hemodialysis because of end-stage kidney disease (n = 377) were excluded. Finally, 2,397 patients were analyzed in the present study. The study design was approved by the Institutional Review Board of Seoul National University Hospital (No. H-2110-085-1262) and complied with the Declaration of Helsinki. The requirement for informed consent was waived by the review board.
Baseline information at the time that CRRT began was collected, such as age, sex, weight, cause of AKI (e.g., septic and nonseptic), initial CRRT settings (e.g., target dose, blood flow rate, and target ultrafiltration), mechanical ventilation, use of vasopressors, the division of intensive care unit, and severity indices (e.g., the sequential organ failure assessment [SOFA], the Acute Physiology and Chronic Health Evaluation [APACHE] II, and the Charlson comorbidity index [CCI]). The SOFA, APACHE II, and CCI scores were calculated using the original formulas [15–17]. Laboratory values, such as pH, potassium, bicarbonate, and phosphate levels, were measured at least twice a day after starting CRRT until the day of VT occurrence or of CRRT discontinuation for patients who did not develop VT. Systolic and diastolic blood pressures were also collected both before and after the VT events.
All patients were monitored with bedside monitors, which produced waveforms of electrocardiograms. VT events were documented in their electronic medical records, and the first VT event was retrospectively collected for the present study. VT was classified as non-sustained VT (NSVT) or sustained VT (SVT) as follows: NSVT, ≥3 consecutive ventricular beats with an R-R interval of 600 ms and lasting <30 seconds; and SVT, a ventricular rhythm of >100 beats per minute lasting ≥30 seconds or requiring termination due to hemodynamic instability.
Outcomes
The primary outcome was all-cause mortality after CRRT, and it was stratified by timeframe (e.g., 7 days, 30 days, and 90 days). Any change in blood pressure during the VT events was additionally evaluated.
Statistical analysis
Categorical and continuous variables are presented as proportions and means ± standard deviations when they were normally distributed and as medians with interquartile ranges when they were not normally distributed, respectively. The normality of the distribution was analyzed using the Kolmogorov-Smirnov test. The chi-square test or Fisher exact test was employed to compare categorical variables. The Student t test or the Mann-Whitney U test was used to analyze continuous variables with or without a normal distribution. The Wilcoxon signed-rank test was carried out to confirm significant changes in continuous variables.
We assessed the effect of VT on mortality outcomes by constructing Kaplan-Meier curves and performing a log-rank test. The hazard ratios and confidence intervals for mortality outcomes were calculated using the Cox proportional hazard regression model. Due to a violation of the Cox proportion assumption, we used a logistic regression model and calculated the odds ratios (ORs) of mortality outcomes with adjustment for multiple variables. The adjusted variables were selected based on the significance of their association with mortality. A competing risk Cox proportional hazard regression model was used at multiple time points of CRRT with time-dependent variables (e.g., pH, potassium, bicarbonate, and phosphate) to investigate the predictors of VT. Time-dependent variables were obtained until VT occurrence or discontinuation of CRRT. All statistical analyses were performed using the IBM SPSS version 27 (IBM Corp.) and R software version 3.5.1) (R Foundation for Statistical Computing). A p-value of <0.05 was considered statistically significant.
Results
Patient demographics
The baseline characteristics are presented in Table 1. The mean patient age was 64 ± 15 years, and 38.6% of the patients were female. The proportion of patients with sepsis was 54.9%. VT occurred in 150 patients (6.3%); most cases took place within 1 week after CRRT initiation (Fig. 1). Patients who developed VT were more likely to require mechanical ventilation or ≥3 vasopressors and had higher SOFA scores than patients without VT.

Baseline characteristics of the patients

A histogram of the occurrence of VT after starting continuous renal replacement therapy.
The line indicates the cumulative occurrence of all the VT events on the right y-axis.
VT, ventricular tachycardia.
The relationship between ventricular tachycardia and mortality
During a median follow-up period of 12 days (interquartile range, 3–29 days), 1,591 patients (66.4%) died. The mortality incidence was 24.3 deaths per 1,000 person-days. When a univariable Cox regression model was applied, several variables, including age, sex, septic AKI, initial CRRT settings (such as blood flow rate and target ultrafiltration), mechanical ventilation, use of ≥3 vasopressors, and SOFA, APACHE II, and CCI scores, were identified as significant factors related to mortality (Table 2), and these variables were included in subsequent multivariable regression models for adjustment.

Unadjusted hazard ratios of all-cause mortality
Fig. 2A shows the Kaplan-Meier survival curves for patients with and without VT, and their survival rates differed (p < 0.001). When VT was classified according to duration, an apparent violation of the proportionality of hazards assumption was observed because the NSVT and non-VT curves crossed (p = 0.97) (Fig. 2B). Similarly, the multivariable regression model confirmed that only SVT was independently associated with a high mortality risk, irrespective of the timeframes (Table 3). Blood pressures were compared before and after the VT events to explore the hemodynamic effects. Although NSVT was not associated with hemodynamic fluctuation, SVT decreased blood pressure, which might be the cause of the high mortality in patients with SVT (Fig. 3).
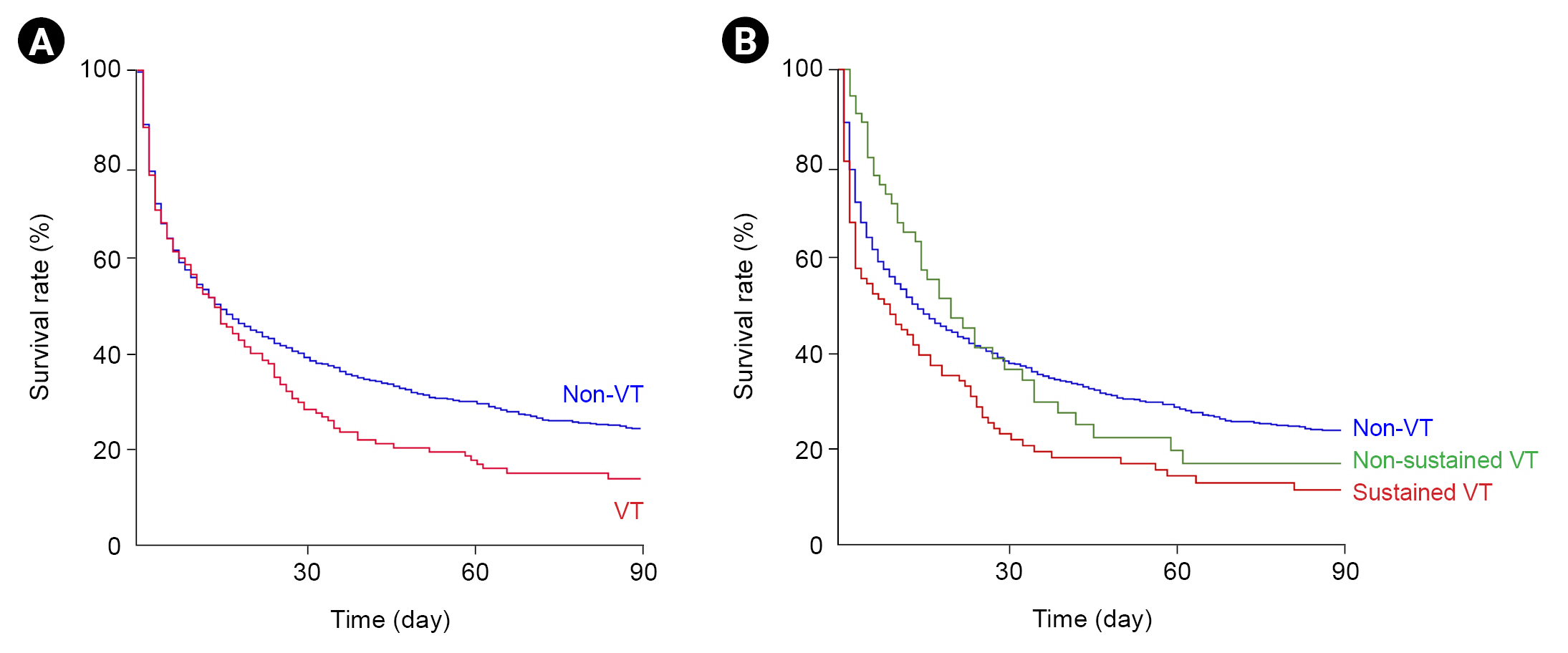
Kaplan-Meier survival curves.
(A) For patients both with and without ventricular tachycardia (VT). (B) VT events are categorized into sustained and non-sustained cases.

Odds ratios of all-cause mortality in patients with ventricular tachycardia compared with those without ventricular tachycardia
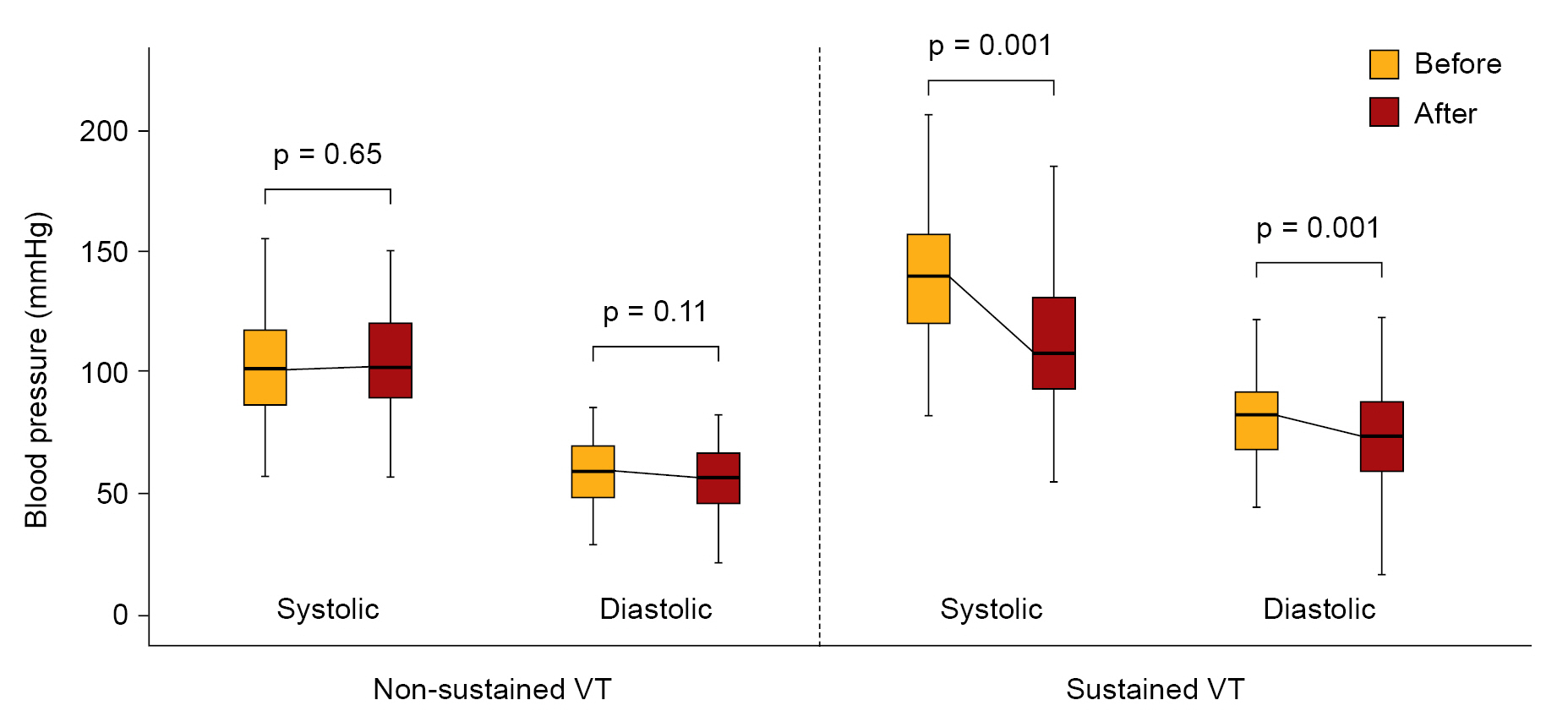
Changes in blood pressure after the occurrence of VT.
VT, ventricular tachycardia.
Risk factors for ventricular tachycardia in patients on continuous renal replacement therapy
Table 4 shows a competing risk Cox regression analysis that was carried out to identify risk factors for either SVT or NSVT. A history of myocardial infarction, vasopressor use, and certain trends, such as acidosis and hyperkalemia, were independently associated with the occurrence of SVT. A history of congestive heart failure and a hypophosphatemia trend were associated with the occurrence of NSVT.

Risk factors for the occurrence of ventricular tachycardia in the multivariable regression model
Discussion
Several arrhythmias may occur after starting CRRT and may exacerbate patients’ existing conditions. The present study focused on VT in patients receiving CRRT, and the occurrence of SVT was associated with worse outcomes, such as a high mortality rate and low blood pressure. Certain factors were correlated with a high risk of VT, such as vasopressor use, acidosis, hyperkalemia, and hypophosphatemia.
A previous study of 595 patients revealed that 2.3% of patients on CRRT had VT [9]. In another multinational cohort of patients treated with CRRT for AKI, VT occurred in 0.2% of patients [6]. The present cohort had a prevalence of 6.3%, and the differences might have depended on the different characteristics of patients in these respective studies. Among all episodes of VT, the incidence of SVT was 4.0%, while that of NSVT was 2.3%. Depending on the definitions for SVT and NSVT, a difference in prevalence might exist between studies [18].
Patients on CRRT frequently require the support of vasopressors because of hemodynamic instability. Vasopressors are generally administered based on the assumption that short-term clinical recovery will be facilitated by an enhanced cardiac output or vascular tone. However, these agents may lead to fatal adverse events, such as sinus tachycardia, asymptomatic ventricular ectopic activity, and other ventricular arrhythmias [19,20]. Our data suggested that the use of many vasoactive agents was associated with an increased risk of SVT, regardless of the severity of illness, which supports the findings reported previously.
According to the time-dependent analysis, hyperkalemia and acidosis were associated with the risk of SVT. Systemic acidosis provokes arrhythmias via both the direct action of Na+-H+ and Na+-Ca2+ exchangers and the indirect action of inflammatory or hyperoxidative injury [21]. Some clinical studies have documented the association between systemic acidosis and VT [22–24]. The presence of systemic acidosis was the strongest determinant of ventricular arrhythmia in patients with ST-elevated myocardial infarction after reperfusion therapy [24]. In addition to the role of hypokalemia as a risk factor for fatal ventricular arrhythmias [25–27], hyperkalemia also exerts effects on cardiac excitability, which predisposes hearts to reentrant tachyarrhythmias, such as VT [28,29]. When combined with hypoxia and acidosis, hyperkalemia promotes phase 2 reentry by further increasing the repolarization reserve in epicardial ventricular tissue [30]. As refractory acidosis and hyperkalemia are frequent complications observed following severe AKI, our data indicate that insufficient dialysis at the early stage of CRRT might be one of the causative factors for VT. Hypophosphatemia, which occurs in 10% to 60% of patients receiving CRRT [31–33], is associated with adverse events, such as prolonged mechanical ventilation or vasoactive agent support in critically ill patients [34,35]. Although an association between NSVT and mortality was not documented in this study, we recommend that phosphate levels be monitored during CRRT because the results of previous studies have demonstrated the potential risk of NSVT [36–38].
Although the current study is informative, certain limitations remain to be addressed. Because of its retrospective design, unmeasured biases and confounders might have interfered with the analyses. Alterations in practice may be related to mortality but were not considered in the present study. The cause of death was not available in the present dataset. Heart function was not thoroughly evaluated, which might be a main cause of VT occurrence. The occurrence of VT and its risk factors may also differ depending on the cause of AKI, but the present study did not categorize nonseptic patients into further specific causes.
The present study indicated that the occurrence of VT in patients on CRRT was associated with an unfavorable prognosis, particularly in those with SVT. Several factors, such as vasopressor use, acidosis, hyperkalemia, and hypophosphatemia, were associated with the risk of VT, and some of them were considered modifiable during CRRT implementation. Accordingly, monitoring VT and making early attempts to reduce the risk factors for VT will therefore be needed after patients begin CRRT.
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.
Data sharing statement
The data are available from the authors upon reasonable request.
Authors’ contributions
Conceptualization: SGK, SSH
Data curation: DY, JL, YSK
Formal analysis: DY, JK, JL, YCK, DKK, KHO, KWJ, HK, YSK
Investigation: DY, JL, MWK, YCK, DKK, KHO, KWJ
Methodology: JK, YCK, HK
Writing–original draft: SGK, SSH
Writing–review & editing: SSH
All authors read and approved the final manuscript.