Staphylococcal infection-associated crescentic immunoglobulin A nephropathy
Article information
A 49-year-old man without a history of chronic disease presented to our hospital with acute fever, dyspnea, and oliguria. His vital signs were: blood pressure 100/60 mmHg, heart rate 120 beats per minute, and body temperature 38.5°C. Laboratory findings were: serum creatinine 2.99 mg/dL, leukocytes 21,230 × 103/μL, hemoglobin 7.6 g/dL, platelets 60,000/μL, and C-reactive protein 183.46 mg/L. Additionally, perinuclear anti-neutrophil cytoplasmic antibody (ANCA) and cytoplasmic ANCA were elevated, and C3 was decreased. However, there were no indications of vasculitis. Computed tomography revealed multifocal pneumonic infiltration along with bilateral cavitary lung lesions and a perirenal hematoma. We initiated empirical antibiotics. Blood cultures revealed methicillin-resistant Staphylococcus aureus, and the patient exhibited signs of uremia, for which he underwent emergency hemodialysis. Echocardiography revealed a tricuspid valve vegetation measuring 2.0 × 0.79 cm. While his renal function and pneumonic infiltration improved after 4 weeks, proteinuria persisted. A renal biopsy showed endocapillary proliferation and increased mesangial immunoglobulin A (IgA) accumulation accompanied by fibrocellular crescents (Fig. 1)–findings typically observed in crescentic IgA nephropathy. We initiated steroid therapy after ensuring complete remission of Staphylococcus infection. The patient’s renal condition stabilized following steroid administration.
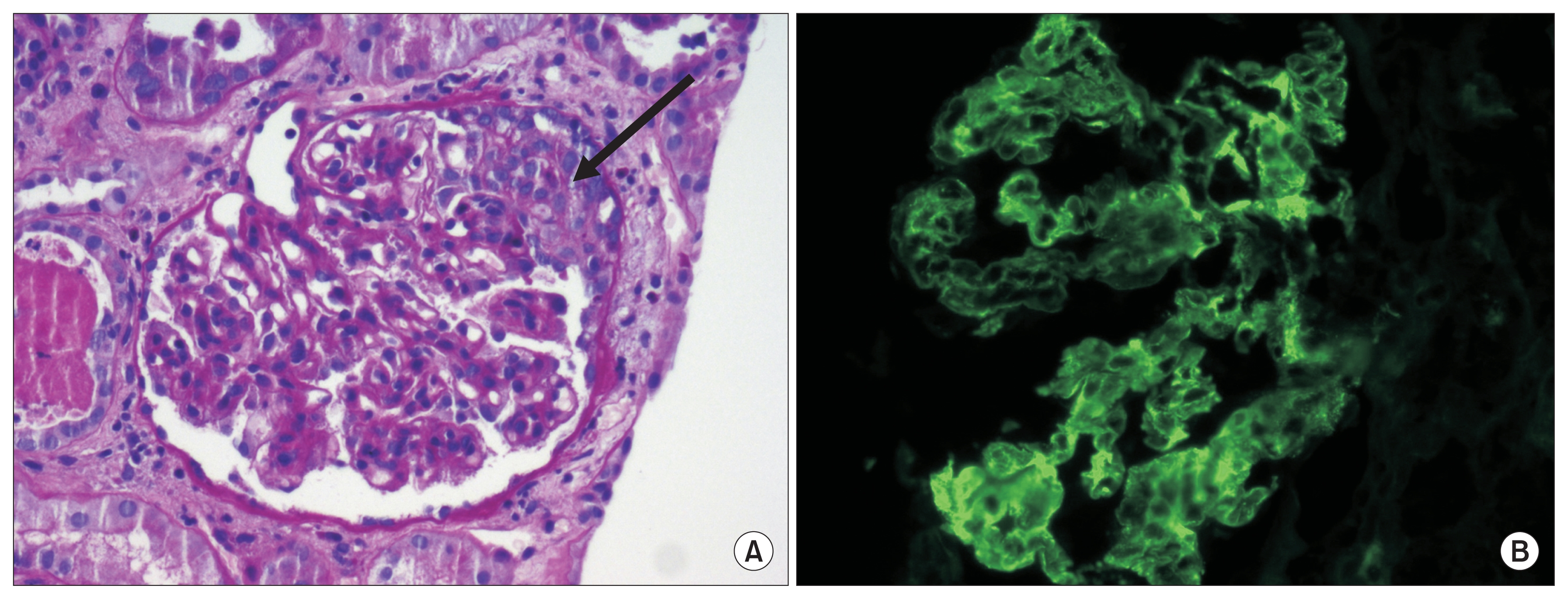
Renal biopsy findings
(A) High-power view showing a fibrocellular crescent (arrow) and endocapillary proliferation combined with mesangial hypercelluarity (hematoxylyn-eosin stain, ×400). (B) Representative image of immunofluorescence showing mesangial infiltration and staining of immunoglobulin A complexes.
Infectious endocarditis often results in proliferative or crescentic glomerulonephritis (GN), primarily presenting as acute kidney injury. Additionally, the histological pattern of Staphylococcus infection-associated GN resembles IgA nephropathy more than other post-infection GN. Thus, Staphylococcus-associated GN mimicking crescentic IgA nephropathy should be considered in the differential diagnosis of cases showing sudden development of azotemia and significant proteinuria in patients diagnosed with staphylococcal endocarditis. However, while steroids form the mainstay of treatment for crescentic IgA nephropathy, Staphylococcus-associated GN is primarily treated with antibiotics. Steroid therapy could be administered following complete remission of infection in patients who demonstrate fibrocellular crescents and severe proteinuria.
Acknowledgments
This work was supported by Wonkwang University in 2017.
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.