


Introduction
Hypertension is the leading global non-communicable cause of mortality and number one risk factor for disability-adjusted life years [1–8]. Further, hypertension is the single largest risk factor for multiple co-morbidities including stroke, myocardial infarction and chronic kidney disease [6,9–12] and is projected to be the principal global cause of death and disability by 2020 [1]. The development of hypertension involves the integration of multiple regulatory systems and as a complex, multifactorial disease, our understanding of the pathogenesis remains elusive. The salt-sensitivity of blood pressure, defined as an exaggerated pressor response to dietary salt intake, affects approximately 50% of hypertensive patients and 25% of normotensive adults [13–17] and profoundly increases the risk of hypertension [13,14,18–20]. The impact of dietary salt intake on blood pressure regulation and the pathogenesis of hypertension is a global public health issue as the average global salt intake of approximately 4 g/day [21–25] significantly exceeds the World Health Organization recommendation of 2 g/day [14]. Critically, despite modifications of the classical renal centric “pressure-natriuresis hypothesis of blood pressure control” [26–28] to include genetic, sympathetic nervous system and renal mechanisms [29–34] our understanding of the role of renal sodium handling in blood pressure regulation is continually expanding. This is highlighted by a recent proposal that neurohumoral control of renal excretory function (i.e., natriuresis) represents the first line of defense against increased salt intake, followed by neurohumoral control of resistance vessels with pressure natriuresis representing a final third line of defense [35]. Therefore, given the central role of renal sodium handling in determining the salt sensitivity of blood pressure increased understanding of the mechanisms influencing renal sodium reabsorption has the potential to identify new therapeutic targets and treatment paradigms for salt-sensitive hypertension. This review is designed to highlight recent advancements in our understanding of the kidney in the etiology and pathogenesis of salt sensitive hypertension.
The genetics of hypertension and sodium handling
The influence of genetics on blood pressure regulation was first modeled in the ‘mosaic theory of hypertension’ [36] and currently hypertension is currently widely acknowledged as a complex polygenic disease state. Over the last several decades approximately 25 rare mutations and over 50 single nucleotide polymorphisms (SNPs) that impact blood pressure have been identified and were reviewed in detail by Padmanabhan et al [32] and presented in an update of the Paige mosaic model of blood pressure regulation. However, given that the majority of genome-wide association studies (GWAS) are not conducted in identified salt-sensitive versus resistant populations the identification of specific genes or markers of the salt-sensitivity of blood pressure has been challenging. Pertinent to this focused review has been the identification of SNPs in the SLC4A5 gene, which encodes the sodium-bicarbonate cotransporter, that correlated with blood pressure in non GWAS studies conducted in 2 separate populations that linked a SNPs to a causal gene (SLC4A5) and the salt-sensitivity of blood pressure [15]. Additionally, recent studies have linked SNP’s in NEDD4L [37] and SNPS located near GNAS, ZNF831 and EDN3 [38] with modulation of the responses to thiazide diuretics—findings which may have direct implications for the personalized use of this class of diuretics in antihypertensive therapy. A recent elegant study provided experimental validation and a mechanistic link between a GWAS identified gene (SH2B3) and renal inflammation in salt-sensitive hypertension. In this study a causal role of SH2B3 was delineated in the pathophysiology of Dahl salt-sensitive (DSS) hypertension. Utilizing zinc-finger nuclease technology Rudemiller et al [39] mutated the SH2B3 gene and observed attenuation of DSS rat hypertension and renal inflammation highlighting the role of this gene in the pathology of salt sensitive hypertension (Table 1). One of the patient cohorts that has been integral in the interrogation of the genetics of salt-sensitivity is the Genetic Epidemiology Network of Salt-Sensitivity Study (GenSalt). This study continues to reveal insights and a recent GWAS study of GenSalt data, confirmed by secondary analysis in the Chinese Multi-Ethnic Study of Atherosclerosis cohort, has provided 8 novel blood pressure loci that are associated with the salt-sensitivity of blood pressure [40].
Three recent publications have provided new evidence of the genetic variations associated with blood pressure. Meta-analysis of 128,272 SNPs in a total population of 432,415 adults including European, Asian and African ancestry has revealed the presence of 66 genome-wide significant blood-pressure associated loci, of which 17 are new [41]. These loci did not strongly associate with a renal target organ effect—suggesting this study did not identify a single dominant locus associated with a predominant negative impact on renal effect. A companion study that conducted the largest ever trans-ancestry meta-analysis of approximately 350,000 subjects identified 30 new blood pressure or hypertension associated loci in the general population [42]—significantly increasing our insight into the impact of genetic on blood pressure variation and potentially providing new therapeutic targets. The final study published by this team of researchers discovered a strong association between cardiometabolic risk and hypertension and identified single-variant associations at 31 new loci using meta-analysis of exome-centric single-variant and gene-based tests for association to blood pressure [43]. Of particular relevance to this review was the association of the aggregation of rare and low-frequency variants in NPR1. NPR1 encodes for atrial and B-type natriuretic peptide that have well defined roles in sodium, volume and blood pressure regulation. However, the functional significance of the low-frequency SNP rs35479618 in NPR1 remains to be established in the context of salt-sensitive hypertension [43]. A caveat to these three large scale genetic studies, in the context of the present review, is the lack of identification of the salt-sensitivity of blood pressure in the tested subjects. Despite these detailed recent advances that expand the number of genetic variants that are associated with blood pressure regulation, most notably in the collection of papers published in Nature Genetics [41–43], the major challenge remains to translate these genetic findings of SNPs into causal gene based molecular mechanisms that can be targeted to expand our ability to treat hypertension.
Inflammation, renal sodium transport and hypertension
Studies from the past two decades have demonstrated that inflammatory cytokines are elevated in hypertensive human subjects, and elevated cytokine levels predict the risk of hypertension in normotensive patients. Although the role of inflammation in the salt sensitivity of blood pressure in humans has not been investigated, multiple animal models of salt-sensitive hypertension are characterized by renal inflammation. The role of infiltrating immune cells in the pathogenesis of salt-sensitive hypertension is highlighted by two recent animal studies. In the DSS rat, depletion of Rag1, a protein critical to the maturation of T and B lymphocytes, reduced the number of circulating T and B lymphocytes in the setting of a normal salt diet. Emphasizing the role of renal immune cell infiltration in response to salt intake, a high salt diet evoked renal T cell infiltration and increased blood pressure in control DSS rats. In contrast, T cell infiltration was reduced and hypertension was attenuated in Rag1-null rats [44]. Further supporting a role for renal immune cell accumulation in the pathophysiology of salt-sensitive hypertension, suppression of T and B lymphocyte proliferation using mycophenolate mofetil blunted dietary sodium-evoked increases in blood pressure and renal macrophage and lymphocyte infiltration and preserved pressure natriuresis in the classical L-NAME model of sodium evoked hypertension in Wistar rats [45].
The study by Franco et al in 2013 [45] directly suggests that renal immune cell infiltration may promote hypertension through alterations in renal sodium handling. Extending and supporting this hypothesis, several studies have delineated mechanistic roles for inflammatory cytokines in the regulation of renal sodium transport. In the context of angiotensin-II (Ang-II)-induced hypertension, both blood pressure and renal sodium retention are dramatically attenuated in mice lacking interferon-γ (IFN-γ−/−) or interleukin 17A (IL-17A−/−). Significantly, Ang-II-mediated increases in the total and phosphorylated forms of the sodium chloride cotransporter (NCC), but not the epithelial sodium chloride transporter (ENaC) are abolished versus attenuated in IFN-γ−/− and IL-17A−/− mice respectively, and the expression of proximal sodium transporters, including the sodium hydrogen exchanger (NHE3) and sodium potassium transporter (NaPi2), are reduced during Ang-II infusion in IFN-γ−/− and IL-17A−/− mice. These data suggest that both of these cytokines contribute to Ang-II hypertension by promoting sodium retention in the distal and proximal nephron [46]. Building upon this body of work, it has been demonstrated that IL-17A influences renal sodium transporter expression and activity in Ang-II hypertension via an SGK1-NEDD4-2 pathway [47]. Highlighting the multitude of cytokines potentially involved in regulating renal sodium transport, Ang-II-induced hypertension and sodium retention are attenuated in mice lacking the IL-1 receptor by a renal macrophage nitric oxide (NO) dependent mechanism that prevents NO-mediated suppression of NKCC2 activity [48]. A direct role for IL-1 in salt-sensitive hypertension is supported by evidence that dietary salt evokes hypertension, NLRP3 inflammasome activation, and caspase-1-mediated cleavage of IL-1β to its mature form in DSS rats. In this established rat model, infusion of a caspase-1 inhibitor into the renal medulla abolished dietary-sodium evoked increases in mature IL-1β levels and attenuated the development of salt-sensitive hypertension [49]. Further, in the DSS rat phenotype, but not in salt-resistant congenic SS.13BN26 rats, dietary salt-evoked hypertension is accompanied by increased tumor necrosis factor (TNF)-α mRNA and protein expression, and renal interstitial infusion of a TNF-α inhibitor, Etanercept, attenuated salt-sensitive hypertension [50]. These mechanistic data, generated in multiple animal models and summarized in Table 2, suggest that renal immune cell infiltration and inflammatory cytokines promote salt-sensitive hypertension by influencing renal sodium handling. Importantly, suppression of immune cell infiltration and renal inflammation promotes sodium homeostasis and normotension and may prove to be a valuable approach to the treatment of salt-sensitive hypertension in human subjects.
Dietary intake and renal sodium handling
Dietary potassium intake has been linked with blood pressure regulation. In particular, clinical data reveals our diet is generally low in potassium and that these associates with elevated blood pressure and salt-sensitive hypertension [51], and the renal handling of potassium and sodium are intrinsically related [52]. Of particular relevance to the salt-sensitivity of blood pressure, a number of recent studies have reported that dietary potassium levels impact sodium reabsorption by modulating the activity of the NCC and ENaC in the distal nephron.
Acute potassium supplementation via oral gavage, intravenous infusion, or ingestion of a potassium-enriched meal rapidly reduces the phosphorylation and activation of the NCC, and these changes are accompanied by significant increases in natriuresis in several mouse strains and in Sprague-Dawley rats [53,54]. Additionally, potassium-evoked natriuresis is blunted in NCC-deficient mice (Sorensen et al [53]). Collectively, these data suggest a critical role of the NCC in mediating the physiological responses (i.e., natriuresis) response to acute increases in total body potassium.
Recent animal studies have provided new insight into the mechanistic links between dietary potassium and salt intake and blood pressure regulation via the NCC. In these studies, a low potassium diet blunted natriuresis and reduced dietary salt-evoked NCC suppression in mice. Further, a low potassium diet was associated with salt sensitivity of blood pressure in wild-type but not NCC-deficient mice, indicating a direct role of the NCC in the effect of dietary potassium on the salt sensitivity of blood pressure [55]. Significantly, expression irrespective of dietary sodium intake a low potassium diet resulted in increased expression and phosphorylation of with-no-lysine kinase (WNK) 4 and increased phosphorylation of SPAK, and OxSR1 [55]. These data suggest that potassium intake directly modulates NCC activity through actions upon its network of regulatory kinases. Elegant cell culture experiments by the same group have demonstrated that the distal convoluted tubule cell is hyperpolarized in the setting of low extracellular potassium, resulting in a decrease in intracellular chloride that activates the NCC via a predominant WNK4–SPAK pathway [55,56]. Despite these novel findings, it is possible that alternative pathways are involved in potassium-mediated regulation of the NCC as potassium-evoked NCC activation is maintained in WNK4 and SPAK knockout mice [57]. These studies have translational relevance, as evidenced by two human studies that have confirmed that a low potassium diet increases the abundance of pNCC in urinary exosomes collected from patients [55,58]. Dietary potassium intake has been recently demonstrated to impact the influence of Ang-II on renal sodium transporter expression in Sprague-Dawley rats. Chronic dietary potassium supplementation did not reduce Ang-II hypertension but attenuated Ang-II-induced upregulation of the NCC but not ENaC [59] suggesting differential actions of potassium on NCC vs. ENaC. The hypothesis of ENaC activation following potassium-induced suppression of sodium retention at the NCC is supported by evidence from studies conducted in mice during acute potassium supplementation [53]. The differential effects of potassium on the NCC and ENaC were highlighted by studies that demonstrated NCC upregulation and activation during low potassium intake and ENaC upregulation during high potassium intake in mice. Importantly, a low potassium-evoked salt sensitivity of blood pressure was abolished by hydrochlorothiazide in these studies [60].
Increasing dietary fructose intake in the typical western diet has mirrored the increasing prevalence of hypertension, and dietary fructose intake is associated with blood pressure in multiple animal studies [61]. In animal models, fructose promotes sodium reabsorption in the kidney, raising the possibility that fructose has a role in the salt-sensitivity of blood pressure. Two recent studies suggest that the mechanism by which fructose promotes salt sensitivity involves the increased activity of the NHE3 in the proximal nephron. Stationary micro-infusion of fructose into the proximal tubules of Wistar rats caused a dose-dependent increase in NHE3 activity, and it was demonstrated both in vivo and in vitro that fructose causes phosphorylation and activation of NHE3 via downregulation of a PKA signaling pathway [62]. In separate studies dietary fructose supplementation prior to and during increased dietary salt intake evokes the development of salt-sensitive hypertension in the salt resistant Sprague-Dawley rat [63]. Companion ex vivo studies of isolated and perfused proximal tubules suggest that 1) fructose stimulates NHE3 activity in a PKC-dependent manner and, 2) that Ang-II mediated-stimulation of NHE3 activity is enhanced by fructose [63]. Together, these studies suggest that a typical Western diet, which features low potassium intake and high fructose and sodium intake, promotes the prevalence salt-sensitive hypertension by modulating renal sodium transporter activity and expression to drive renal sodium retention (Table 3).
Reactive oxygen species and salt sensitivity
NO and reactive oxygen species (ROS) reciprocally alter pressure-natriuresis, and a shift in redox balance in the kidney has been implicated in human hypertension and in multiple animal models of hypertension [64]. Highlighting the importance of NO production in the maintenance of sodium balance and normotension, collecting duct-specific knockout of all isoforms of nitric oxide synthase 1 (NOS1) in mice causes sodium retention and salt-sensitive hypertension [65]. While NOS1α knockout mice do not exhibit hypertension or salt sensitivity of blood pressure, pharmacological inhibition of NOS1β in both wild-type and NOS1α knockout mice induces salt-sensitive hypertension and blunts the natriuretic and diuretic responses to an acute volume expansion, indicating a specific role for NOS1β in natriuresis and salt sensitive hypertension [66]. Recent studies indicate that NO influences the salt sensitivity of blood pressure through several independent mechanisms. Building upon an established body of literature demonstrating that NO regulates renal sodium transporter activity [67], two studies have reported that NO production is impaired in Ang-II hypertension [68], and that exogenous NO restores endothelin 1-evoked inhibition of NKCC2 activity in this model [69]. Beyond modulation of renal sodium transporters dietary salt-evoked upregulation of NOS1β in the macula densa reduces tubuloglomerular feedback responsiveness to promote sodium excretion. Significantly, macula densa-specific knockout of NOS1β results in salt-sensitive hypertension [70], indicating that NO may also influence salt sensitivity by modulating renal hemodynamic auto-regulation.
Beyond direct effects of NO renal oxidative stress and inflammation accompany salt-sensitive hypertension in mice deficient in manganese superoxide dismutase [71], and renal levels of ROS hydrogen peroxide are elevated in DSS rats during high salt intake [72]. Elegant in vivo studies have shown null mutation of the p67phox subunit of NADPH oxidase, a major source of ROS, attenuates hypertension in the DSS rat, and that dietary salt intake evokes a reduction in renal medullary blood flow and glomerular filtration rate that is blunted in p67phox-null mice [73]. Together, these studies suggest that elevated renal ROS production may contribute to salt sensitive hypertension by reducing sodium delivery and filtration in the kidney, thereby promoting sodium retention. Surprisingly, dietary salt-evoked generation of ROS by NADPH oxidase blunts myogenic autoregulation of renal blood flow and glomerular filtration rate in the salt-resistant Sprague-Dawley rat. These apparently contradictory findings raise the intriguing possibility that ROS may play an important physiological role in promoting renal sodium excretion and the maintenance of salt resistance [74].
The sympathetic nervous system and renal sodium handling
It has recently been reported in a high profile study that salt-sensitive hypertension is driven by increased renal sympathetic nerve release of norepinephrine (NE) which evokes NCC up regulation through a WNK4-β2 adrenoceptor pathway [75]. However, the lack of a reproducible role for β2-adrenoceptors on NCC regulation in vivo in mice [76] and evidence of 1) an acute synergistic role of α- and β-adrenoceptors on NCC expression [77], 2) a key role of WNK1 in mediating NCC activation [78], and 3) lack of increased NCC expression and activity in rats during long term NE infusion [79] challenge this hypothesis. Owing to this ongoing controversy of the direct effect of sympathetic outflow, which is increased in several forms of hypertension, the impact of systemic and local release of NE on the regulation, expression and activity of the NCC requires further investigation.
The impact of the renal sympathetic nerves in the long-term regulation of blood pressure, via mechanisms that impact renal sodium reabsorption has been established for several decades. However, these classical studies, and recent human renal nerve ablation trials which demonstrated significant reductions in blood pressure in small highly controlled studies and no effect in large scale multi-center blinded trial [80–82], removed the influence of both afferent (from kidney) and efferent (to kidney) renal nerves. To address the individual actions of the afferent renal nerves a method of selective ablation of the renal afferent nerves, utilizing periaxonal capsaicin treatment has been developed in rats [83]. This technique selectively disrupts the afferent but not efferent renal nerves to provide a new tool with which to examine the contribution of the afferent renal nerves to hypertension. Removal of the afferent renal nerves prior to graded chronic increases in dietary sodium intake in the Sprague-Dawley rat suggest that the renal afferent nerves are not essential to maintain sodium homeostasis and blood pressure in this paradigm. In the classical rat model of salt sensitive hypertension, the DSS rat, recent studies show that bilateral renal denervation (removing both efferent and afferent nerves) in hypertensive animals reduces blood pressure [84] and that this effect is observed following short and long-term hypertension [85]. Further, this effect is efferent nerve mediated as selective afferent nerve ablation did not alter blood pressure. In contrast, the renal afferent nerves play a role in the full development of deoxycorticosterone acetate-salt hypertension, with afferent nerve ablation and bilateral renal denervation attenuating the magnitude of hypertension by approximately 50% [86]. However, in these studies only removal of the efferent nerves prevented a renal inflammatory response. This finding of a role of the efferent, but not afferent renal nerves in renal inflammation is supported by recent evidence that bilateral renal denervation, but not selective removal of the afferent renal nerves, attenuates Ang-II hypertension and inflammation [87]. These data collectively suggest that the differential impact of the afferent versus efferent nerves on blood pressure regulation may depend on the underlying cause of hypertension and has implications for the application of renal nerve ablation in humans.
Conclusion
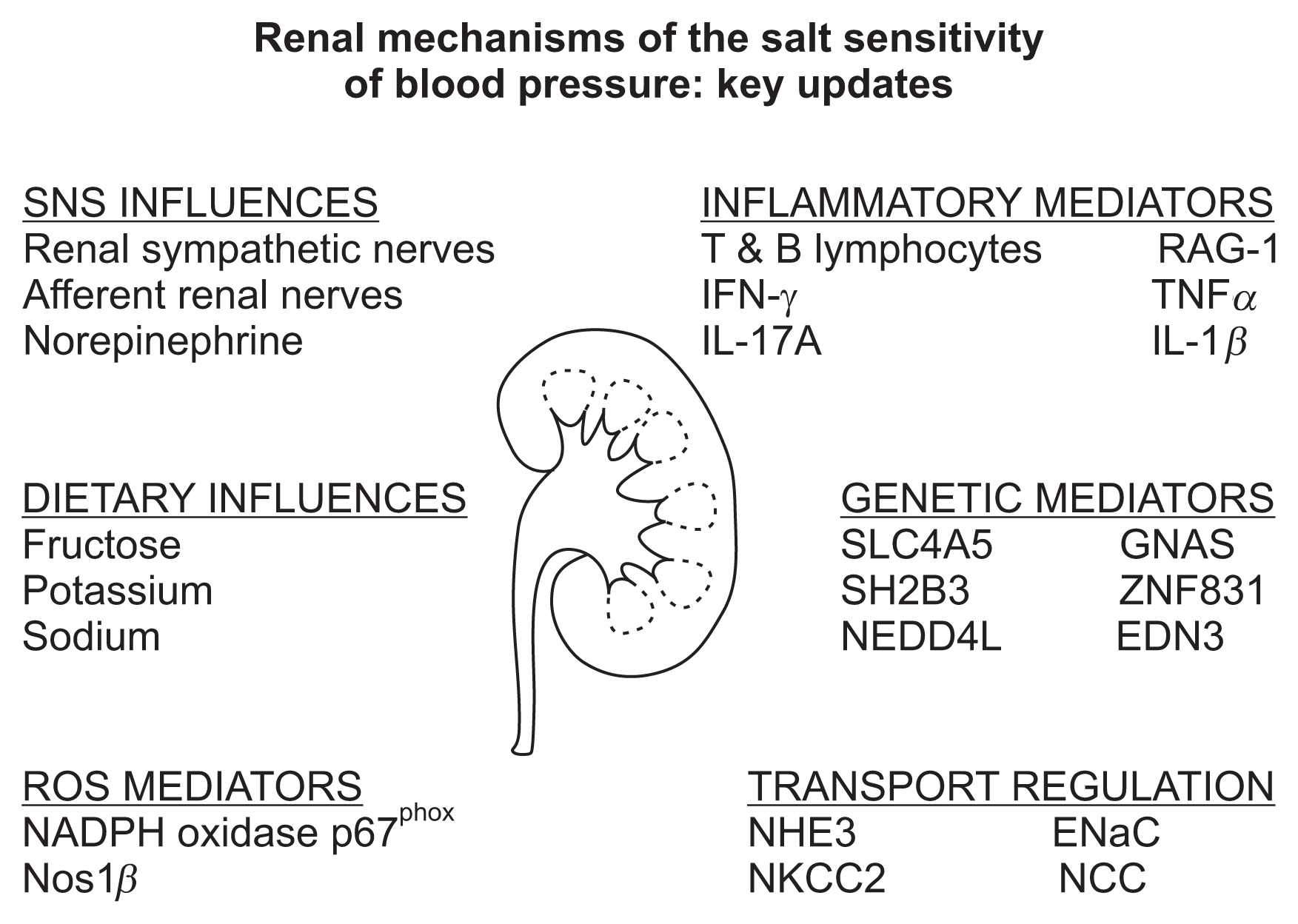
Over the last several years, our understanding of the mechanisms that influence the renal handling of sodium and the salt sensitivity of blood pressure has dramatically increased through novel discoveries in both the basic science and genetic based clinical arenas. These findings have solidified the role of kidney as a predominant mechanism regulating blood pressure via the modulation of renal sodium excretion in multiple hypertensive disease states. The advances outlined in this review and summarized in Fig. 1 have revealed an increasingly important role of the influence of inflammatory pathways and dietary composition on renal sodium handling. Further, the recent discoveries of multiple new genes that influence both blood pressure and salt sensitivity provides an exciting opportunity to conduct casual mechanistic studies which have profound potential to increase our understanding of both renal function and hypertension. Recent basic science studies have highlighted a role of the renal sympathetic nerves in the regulation of both inflammation and renal sodium transporter activity—suggesting that depending on the underlying cause of hypertension renal nerve ablation may represent a suitable therapeutic approach. We expect the next few years will provide further delineation of the mechanisms influencing renal sodium reabsorption and will potentially identify cross talk between these pathways in the regulation of sodium homeostasis and blood pressure (i.e., genetic influences on inflammation that regulate renal sodium transport expression). We speculate that the ongoing identification and interrogation of mechanism based casual genetic pathways, inflammatory mediators, renal sympathetic nerve pathways and dietary influences on renal sodium handling will generate new therapeutic targets and refinements to current dietary guidelines that will have broad applications in the treatment of human hypertension.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









