

Focus of issue
- Page Path
-
- HOME
- BROWSE ARTICLES
- Focus of issue
| ||
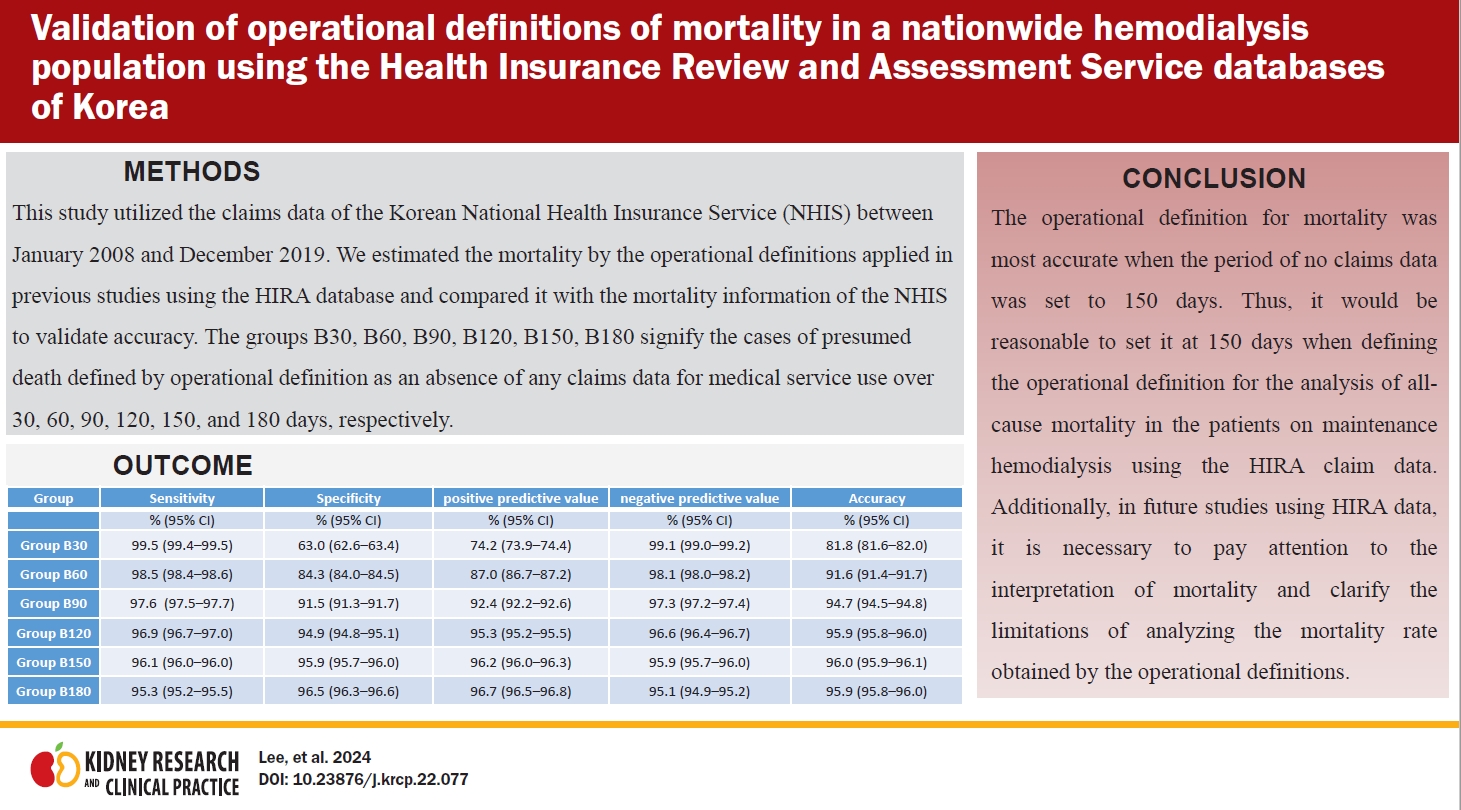
| This study aimed to validate operational definitions of mortality for maintenance hemodialysis patients that have been used when analyzing the Korean Health Insurance Review and Assessment Service (HIRA) database. Authors estimated mortality based on operational definitions applied in previous studies using the HIRA database and compared it with NHIS mortality information to validate accuracy. A total of 128,876 patients who started maintenance hemodialysis between January 2009 and December 2019 were analyzed. The accuracy of estimated mortality was the highest at 96% in the group where mortality was defined as an absence of claims data for 150 days. If the period of no claims data was set to 90 days or less, there was a risk of overestimating the mortality for the entire study period. When it was set to 180 days or more, there was a risk of underestimating the mortality, as the follow-up time was close to the end of the study period. When mortality analysis of maintenance hemodialysis patients is performed using HIRA data, it is most accurate to set the operational definition period as the absence of claims data for 150 days. | ||
 | ||
| ||
| This study aimed to address this gap by investigating the characteristics of glomerular diseases following the COVID-19 infection and vaccination in South Korea. Data from multiple centers were used to identify de novo glomerulonephritis (GN) cases with suspected onset following COVID-19 infection or vaccination. Glomerular diseases occurred shortly after the infection or vaccination. The most prevalent postinfection GN was podocytop¬athy (42.9%), comprising primary focal segmental glomerulosclerosis and minimal change disease, whereas postvaccination GN mainly included immunoglobulin A nephropathy (IgAN; 57.9%) and Henoch-Schönlein purpura nephritis (HSP; 15.8%). The proportion of glomerular diseases changed during the pandemic in South Korea, with an increase in acute interstitial nephritis and a decrease in pauci-immune crescentic GN. This study showed the characteristics of GNs following COVID-19 infection or vaccination in South Korea. | ||
 | ||
| ||
| This study evaluated the association between estimated glomerular filtration rate (eGFR) or albumin¬uria and the risk of death from diverse causes. Authors screened >10 million general health screening examinees who received health examinations conducted in 2009 using the claims database of Korea. The primary outcome was mortality and cause-specific death between 2009 and 2019 identified through death certificates based on the diagnostic codes of International Classification of Diseases, 10th revision. The hazard ratio of death was significantly high in both the eGFR <60 mL/min/1.73 m2 and in the eGFR ≥120 mL/ min/1.73 m2 groups in univariable and multivariable regression analyses when compared to those within the reference range (eGFR of 90–120 mL/min/1.73 m2). The results were similar for death by cardiovascular, cancer, infection, endocrine, respiratory, and di¬gestive causes. They also found that albuminuria was associated with higher risk of death regardless of eGFR range, and those in the higher categories of dipstick albuminuria showed higher risk. This study reconfirmed the significant association between eGFR, albuminuria, and mortality. | ||
 | ||


-
Kidney Research
and
Clinical PracticePrint ISSN: 2211-9132
Online ISSN: 2211-9140
-


-
Impact Factor3.0
-
-
-

-




")








- Editorial Office
-
#301, (Miseung Bldg.) 23, Apgujenog-ro 30-gil, Gangnam-gu, Seoul 06022, Korea
Tel: +82-2-3486-8736 Fax: +82-2-3486-8737 E-mail: registry@ksn.or.kr
Copyright © 2024 by The Korean Society of Nephrology.

