



A COVID-19 outbreak in Korean hemodialysis units
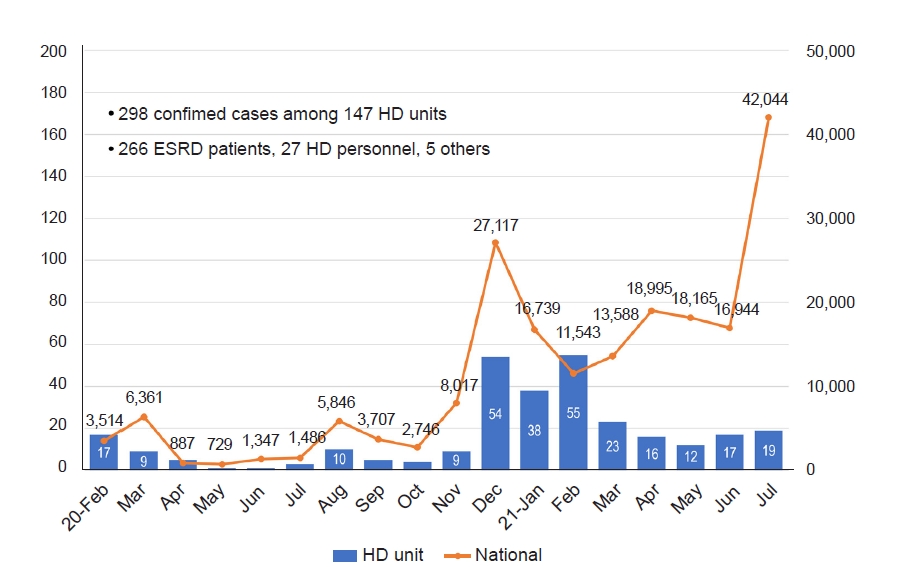
Coronavirus disease 2019 (COVID-19) has spread rapidly and resulted in nearly 2 billion confirmed cases and more than 4 million deaths worldwide. Accordingly, 198,345 confirmed cases and 2,095 deaths had occurred in Korea, by July 2021. Since we have experience coping with Middle East respiratory syndrome [1,2] and have developed infection control guidelines for hemodialysis (HD) units [3], the Korean Society of Nephrology (KSN) established a COVID-19 Task Force Team (COVID-19 TFT) when the first case of COVID-19 was confirmed in Korea. As a result, the number of infections in HD units did not increase significantly. Through July 2021, 298 confirmed patients from 147 HD units were diagnosed with COVID-19, including 266 patients with end-stage renal disease (ESRD) and 27 healthcare workers (Fig. 1).
The role of the COVID-19 TFT during the outbreak
The role of our COVID-19 TFT includes (1) development of and updates to COVID-19 clinical practice guidelines for HD units, (2) distribution of medical resources such as manpower, equipment, and facilities throughout the nephrology network, (3) policy proposal to government authorities, and (4) establishment of an international cooperative network to cope with the COVID-19 pandemic.
The COVID-19 TFT developed the first draft of clinical practice guidelines for preventing secondary transmission of COVID-19 in HD units [4]. The first draft of these clinical practice guidelines was published on January 31, 2020, far before the first HD case was confirmed. There have been several updates since the first draft was published, and the sixth edition of the clinical practice guidelines currently is used in Korean HD facilities. During the COVID-19 outbreak in the Daegu and Gyeongbuk provinces from February to March 2020, 11 HD patients and seven healthcare workers in 11 dialysis units were infected with COVID-19. However, with strict adherence to the COVID-19 clinical practice guidelines and implementation of cohort isolation, the secondary transmission rate was only 0.66% [5].
Another role of our COVID-19 TFT is to distribute medical resources among outbreak regions and to prevent medical burnout in HD units. The COVID-19 TFT helped the government to designate hospitals able to offer HD treatment in isolation. When a confirmed case developed in one HD unit, the COVID-19 TFT contacted the associated hospital through an online chatroom and communicated with the central headquarters to transfer the confirmed case immediately. In addition, when there was a shortage of doctors and nurses to care for the patients, the COVID-19 TFT sent a letter to the members of the KSN to volunteer for isolation care. When the nephrologist position became vacant at the Good Samaritan Bagae Hospital, the first designated private hospital, KSN members volunteered to treat COVID-19-positive, dialysis-dependent patients. To prevent medical burnout, the COVID-19 TFT suggested a de-isolation strategy to return recovered patients to the original HD unit at the proper time (Table 1).
Third, our COVID-19 TFT was responsible for proposing adequate policies to the government. The team requested that the government authority restrict the movement of patients during the outbreak, provide transportation for self-quarantined patients, and supplement adequate personal protective equipment necessary for quarantine dialysis. The COVID-19 TFT also requested timely COVID-19 testing for suspected patients currently receiving HD so as not to delay their essential HD treatment. We also asked the government to reimburse COVID-19-affected hospitals for the additional workload, such as additional shifts, cohort isolation care, and overtime work. Finally, our team requested that the government prioritize vaccine distribution for patients with ESRD and posted the COVID-19 vaccine recommendations in reference to the COVID-19 vaccine statement from the United States [6,7]. As a result, our patients received COVID-19 vaccines earlier than other populations. As of July 2021, 40,489 patients (61.4%) with ESRD were vaccinated fully. This metric is comparable to those of nursing homes (72.6%) and medical practitioners (66.4%); the overall vaccination rate is 13.9% [8].
Finally, the COVID-19 TFT shared our experience with COVID-19 among other countries. Since we have successfully controlled the transmission of COVID-19 without closing any HD units, renal communities in other countries have contacted us to learn our methods to prevent further transmission of COVID-19. Through online webinars, we have shared our experiences for preventing further infections in HD units and the importance of establishing a joint committee to deal with outbreaks.
Future challenges
Although patients who receive in-center HD are at higher risk of acquiring COVID-19, it is impossible to lockdown the HD unit because such treatment is essential for patient survival. Therefore, continuation of uninterrupted dialysis services while adhering to infection prevention guidelines is critical. Along with KSN members, the COVID-19 TFT will make every effort to protect our HD patients and medical staff from the threat of COVID-19.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









