



Introduction
Chronic kidney disease (CKD) is a global health problem that imposes socio-economic burdens on the medical care system [1–3]. Risk stratification for cardiovascular (CV) disease in patients with CKD is an issue of particular importance, as coronary artery disease (CAD), along with heart failure, is a leading cause of mortality and morbidity [4,5]. The risk of CAD is increased even in the early stages of CKD [6] and is further aggravated by the progression of CKD [7]. Because CKD staging is usually determined by the estimated glomerular filtration rate (eGFR) [8], the relationship between renal tubule function and the risk of CAD in this population is poorly understood.
Chloride is the most abundant anion in extracellular fluid and is delicately handled by specific channels and transporters [9,10]. The clinical investigation of urine chloride has been limited to the assessment of volume status [11] and calculation of anion gap [12], until a recent study reported associations of urinary chloride concentration with renal outcomes in patients with nondialysis CKD [13]. Based on the key finding that low urinary chloride concentration was significantly associated with an increased risk of CKD progression, the results suggested that adequate urinary chloride excretion may reflect functionally intact renal tubules [13]. Yet, to our best knowledge, the association between urinary chloride excretion and the risk of CAD has never been validated.
Assessments of coronary artery calcification (CAC) by cardiac computed tomography (CT) scans sensitively detect CAD, and have been validated for prediction of future CV events [14–17]. Taking advantage of the availability of cardiac CT images at baseline and 4-year follow-up for a sample of 1,065 patients with nondialysis CKD, we investigated the relationships between urinary chloride excretion and progression of CAC. We hypothesized that high urinary chloride excretion is associated with decreased risk of CAC progression. In addition, we conducted a series of subgroup analyses to determine whether the relationships between urinary chloride excretion and the risk of CAC progression are modified by clinical context.
Methods
Study design
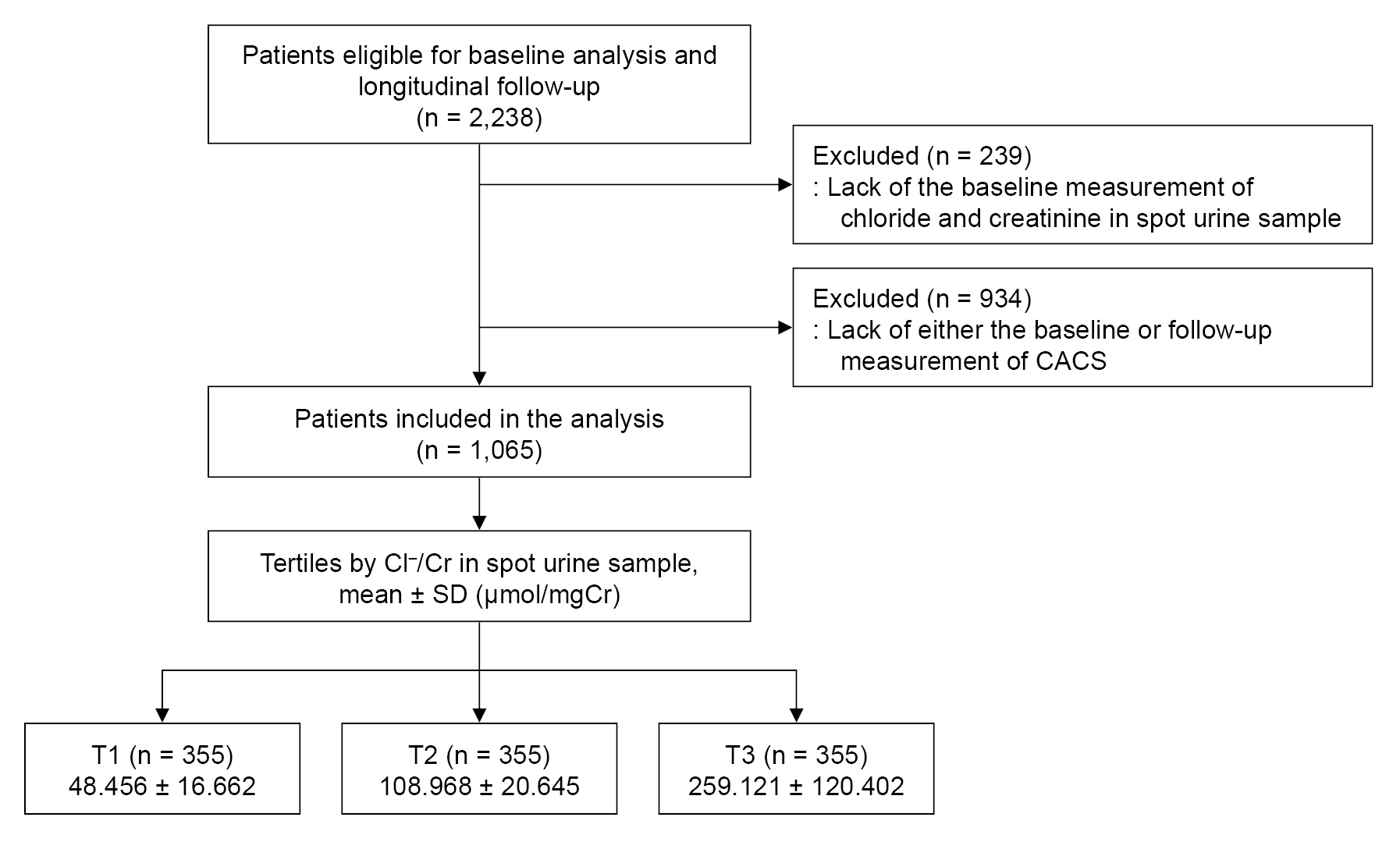
The Korean Cohort Study for Outcomes in Patients With Chronic Kidney Disease (KNOW-CKD) is a nationwide prospective cohort study involving nine tertiary-care general hospitals in Korea (NCT01630486 at https://www.clinicaltrials.gov) [18]. Korean patients with CKD from stage 1 to predialysis stage 5 who voluntarily provided informed consent were enrolled from 2011 through 2016. The study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Boards of participating centers, including Seoul National University Hospital (No. 1104-089-359), Yonsei University Severance Hospital (No. 4-2011-0163), Kangbuk Samsung Medical Center (2011-01-076), The Catholic University of Korea, Seoul St. Mary’s Hospital (No. KC11OIMI0441), Gil Hospital (No. GIRBA2553), Eulji General Hospital (No. 201105-01), Chonnam National University Hospital (No. CNUH-2011-092), and Inje University Busan Paik Hospital (No. 11-091). All participants had been under close observation, and participants who experienced study outcomes were reported by each participating center. Among 2,238 participants who were longitudinally followed up, excluding those lacking baseline measurements of chloride and creatinine (Cr) in spot urine samples, and excluding those lacking either baseline or follow-up measurements of coronary artery calcium score (CACS), a total of 1,065 subjects were finally included in the analyses (Fig. 1).
Data collection from participants
Demographic information was collected from all eligible participants, including age, sex, comorbid conditions, primary renal disease, smoking history, and medication history (angiotensin-converting enzyme inhibitor [ACEi]/angiotensin II receptor blockers [ARBs], diuretics, number of anti-hypertension drugs, statins). Trained staff members measured the heights and weights of study participants. Body mass index (BMI) was calculated as weight divided by height squared. Systolic and diastolic blood pressures (SBP and DBP) were measured by an electronic sphygmomanometer after seated rest for 5 minutes. Venous samples were collected following overnight fasting, to determine hemoglobin, albumin, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), fasting glucose, high-sensitivity C-reactive protein (hsCRP), 25-hydroxyvitamin D (25(OH) vitamin D), sodium, potassium, chloride, and Cr levels at baseline. eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation [19]. CKD stages were determined by the Kidney Disease Improving Global Outcomes guidelines [8]. Urine albumin-to-Cr ratio (ACR) was measured in random, preferably second-voided, spot urine samples. Other urinary metrics, such as sodium, potassium, chloride, and Cr, were also measured in spot urine samples at baseline.
Measurement of coronary artery calcium score
Electrocardiography-gated coronary multidetector CT scans were checked following the standard protocol of each center at baseline and at year four follow-up visits. The CACS score was determined using Agatston units (AU) on a digital radiologic workstation [20].
Exposure and study outcome
The exposure of primary interest was urinary chloride-to-Cr ratio (Cl–/Cr), which was used as a categorical variable. The subjects were divided into tertiles (T1, T2, and T3) by spot urine Cl–/Cr. T1, T2, and T3 were defined as low, moderate, and high urinary chloride excretion, respectively. The study outcome was progression of CAC, which was defined as increase in CACS of more than 200 AU during the 4-year follow-up period, as in previously published studies from KNOW-CKD [21–23].
Statistical analysis
Continuous variables were expressed as the mean ± standard deviation or median (interquartile range). Categorical variables were expressed as the number of participants and percentage. Normality of distribution was ascertained by the Kolmogorov-Smirnov test. To compare baseline characteristics by urinary Cl–/Cr, one-way analysis of variance and chi-square test were used for continuous and categorical variables, respectively. Univariate correlation analysis was performed with Spearman correlation analysis to assess the relationship between urine electrolyte parameters. Participants with any missing data in the primary analysis were excluded from further analyses. Binary logistic regression models were analyzed to address independent associations between urinary chloride excretion and the risk of CAC progression. The results of binary logistic regression models are presented as odds ratios (ORs) and 95% confidence intervals (CIs). Models were constructed after adjusting for the following variables. Model 1 represents crude ORs. Model 2 was adjusted for age, sex, Charlson comorbidity index, primary renal disease, current smoking status, medication (ACEi/ARBs, diuretics, number of antihypertensive drugs, statins), BMI, and SBP. Model 3 was further adjusted for hemoglobin, albumin, fasting glucose, HDL-C, TG, 25(OH) vitamin D, hsCRP, eGFR, and spot urine ACR. Model 4 was additionally adjusted for CACS at baseline. Restricted cubic splines were used to visualize the associations between urinary chloride excretion as a continuous variable and the OR for CAC progression. To validate our findings, we performed sensitivity analyses. First, participants with CACS of 0 AU at the baseline were excluded from binary logistic regression analysis, as CAC progression in those subjects was relatively rare. Second, we excluded subjects with eGFR of <15 mL/min/1.73 m2, because there were relatively few subjects with eGFR of <15 mL/min/1.73 m2, and including them may exaggerate the association between urinary chloride excretion and study outcomes due to advanced CKD. Third, we excluded subjects with eGFR of ≥90 mL/min/1.73 m2, because those values are close to normal kidney function, and may not represent the CKD population well. Fourth, spot urine Na+/Cr and K+/Cr were included as covariates in binary logistic regression analysis. Lastly, we replaced the missing values in primary analyses by multiple imputations, and further conducted Cox regression analyses. To examine whether the association of urinary chloride excretion with the risk of CAC progression is modified by clinical contexts, we conducted prespecified subgroup analyses. Subgroups were defined by age (<60 years vs. ≥60 years), sex (male vs. female), BMI (<23 kg/m2 vs. ≥23 kg/m2), eGFR (<45 mL/min/1.73 m2 vs. ≥45 mL/min/1.73 m2), and spot urine ACR (<300 mg/gCr vs. ≥300 mg/gCr). Two-sided p-values of <0.05 were considered statistically significant. Statistical analysis was performed using IBM SPSS for Windows version 22.0 (IBM Corp.) and R version 4.1.1 (R project for Statistical Computing).
Results
Baseline characteristics
The baseline characteristics of the study participants are described by tertiles of spot urine Cl–/Cr (Table 1). BMI was highest in T3 and lowest in T1. The proportion of subjects using diuretics was highest in T1 and lowest in T3. The eGFR at baseline was highest in T3, and lowest in T1. Accordingly, the proportion of subjects in advanced stages of CKD was higher in T1. The other variables, including CACS at the baseline, did not show significant differences across groups. Correlation analysis to assess the relationships between urine electrolyte parameters revealed significant correlations among urinary sodium, potassium, and chloride excretion (Supplementary Table 1, available online).
Association of spot urine Cl–/Cr and risk of coronary artery calcification progression in patients with nondialysis chronic kidney disease
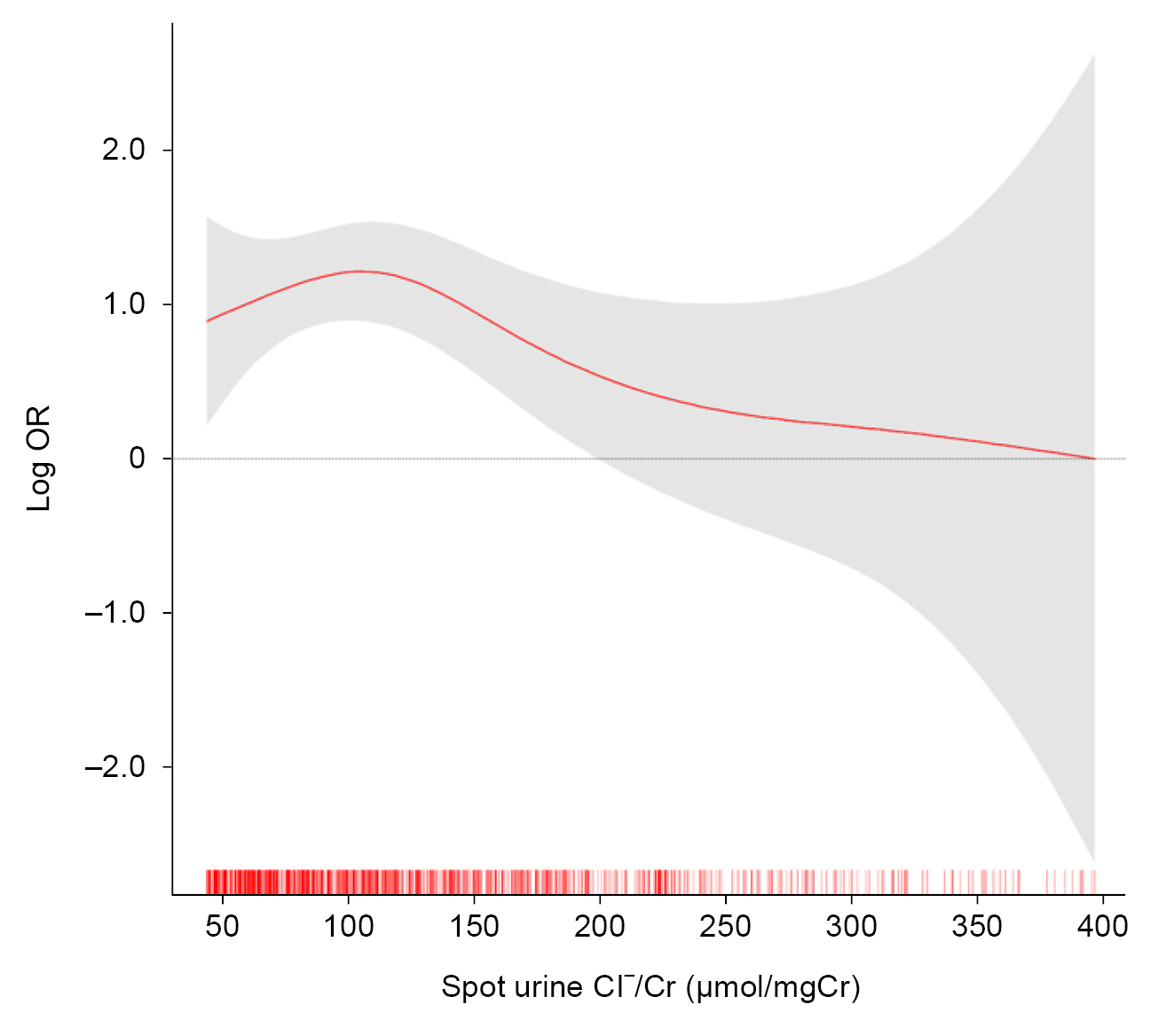
To determine independent associations of spot urine Cl–/Cr with the risk of CAC progression, we analyzed a binary logistic regression model (Table 2). Compared to moderate urinary chloride excretion, high urinary chloride excretion was associated with decreased risk of CAC progression (adjusted OR, 0.38; 95% CI, 0.19–0.76). Low urinary chloride excretion was not associated with either increased or decreased risk of CAC progression (adjusted OR, 0.72; 95% CI, 0.39–1.34). Restricted cubic spine depicted an inverted J-shaped curve, with a significant reduction of the risk for CAC progression in subjects with high spot urine Cl–/Cr (Fig. 2).
Sensitivity analyses
After excluding subjects with CACS of 0 AU at baseline, high urinary chloride excretion was still associated with decreased risk of CAC progression (adjusted OR, 0.36; 95% CI, 0.17–0.72) (Table 3). After excluding subjects at CKD stage 1, the association between high urinary chloride excretion with decreased risk of CAC progression was still significant (adjusted OR, 0.34; 95% CI, 0.16–0.74) (Supplementary Table 2, available online). After excluding subjects at CKD stage 5, the association between high urinary chloride excretion with decreased risk of CAC progression was still robust (adjusted OR, 0.37; 95% CI, 0.18–0.74) (Supplementary Table 3, available online). Even when spot urine Na+/Cr and K+/Cr were included in the regression model as covariates, the analysis demonstrated robust results (Supplementary Table 4, available online). Lastly, after replacing the missing values by multiple imputations, the association between high urinary chloride excretion with decreased risk of CAC progression remained robust (adjusted OR, 0.40; 95% CI, 0.20–0.78) (Supplementary Table 5, available online).
Subgroup analyses
Subgroup analyses revealed that the association of urinary chloride excretion with the risk of CAC progression is not modified by age, sex, BMI, eGFR, or albuminuria (Table 4).
Discussion
In the present study, we demonstrated that high urinary chloride excretion is associated with decreased risk of CAC progression in patients with nondialysis CKD. The association depicted an inverted J-shaped relation, with a significant reduction of the risk for CAC progression in subjects with high spot urine Cl–/Cr. Subgroup analyses revealed that the association is not modified by age, sex, BMI, eGFR, or albuminuria.
Urinary sodium and potassium excretion are correlated with dietary sodium and potassium intake, respectively [24,25]. As high urinary sodium or low urinary potassium excretion was associated with adverse CV outcomes in patients with CKD [25,26], it is interesting that the impact of urinary chloride excretion on the risk of CAC progression was not neutralized, considering that chloride ions are coupled with both sodium and potassium ions. This suggests that urinary chloride excretion does not simply estimate dietary chloride intake, and, rather, may represent the result of renal tubular handling of chloride ions that reflects distal delivery of chloride.
We speculate that adequate urinary excretion of chloride is a result of preserved renal function, thereby contributing to the prevention of CAC progression. A possible mechanism explaining how urinary chloride excretion guarantees a renoprotective effect is tubuloglomerular feedback (TGF) [27]. TGF is an autoregulatory mechanism that controls glomerular filtration rate (GFR). Increased distal flow, and corresponding increased distal delivery of chloride ions, is sensed by macula densa cells, leading to the release of adenosine from their basolateral sides, which in turn causes the constriction of glomerular afferent arterioles [27–29]. This collectively prevents unopposed increases in GFR, and assists in the maintenance of intratubular flow rate. From the perspective of pathophysiology, the activation of TGF functions as a defensive mechanism against glomerular hypertension, which has been shown to be effective in the long-term preservation of GFR [30–33]. Although increased delivery of sodium ions may also initiate TGF response, animal studies demonstrated the predominant role of chloride, rather than sodium, ions as stimulation for macula densa cells to drive TGF [28,34]. It is assumed that, therefore, adequate activation of TGF response is mirrored in high urinary chloride excretion, ultimately contributing to the preservation of kidney function, and to the prevention of CAC prevention. We speculate that the predictive value of urinary chloride excretion as a biomarker of CAC progression is substantial, because despite there being no association between urinary chloride excretion and CACS at baseline, the risk of CAC progression significantly differed by baseline urinary chloride excretion in 4 years.
It is well-known that the risk of CAD is increased even in the early stages of CKD [6], while the risk is further aggravated by progression of CKD [7], which is usually determined by eGFR [8]. Although urinary chloride excretion is postulated to be a biomarker of renal tubule function, we found that it was also correlated with eGFR (Table 1), suggesting that the function of the renal tubule is closely related to that of the glomerulus. Thus, it seems reasonable that urinary chloride excretion predicts the risk of CAC progression. Nevertheless, it is still intriguing that the regression models in the current study include eGFR as a co-variable, which means that the association of urinary chloride excretion with the risk of CAC progression is independent of eGFR. It should be, therefore, further clarified whether the primary defect in renal tubular handling of chloride excretion may increase the risk of CAC progression.
Several limitations are to be acknowledged in the current study. First, we cannot determine a causal relation between urinary chloride excretion and the risk of CAC progression, because of the observational nature of the current study. Second, despite the robust findings for the association between urinary chloride excretion and the risk of CAC progression, we were not able to identify the precise mechanism underlying the association. Third, we did not examine whether urinary chloride excretion is also associated with the overall CV outcomes in patients with nondialysis CKD. Fourth, as this cohort study enrolled only ethnic Koreans, precautions are required to extrapolate the data to other populations.
In conclusion, we report that high urinary chloride excretion is associated with decreased risk of CAC progression in patients with nondialysis CKD. Further studies are warranted to unveil the precise mechanism underlying the association between urinary chloride excretion and the risk of CAC progression and to determine whether urinary chloride excretion is also associated with overall CV outcomes in patients with nondialysis CKD.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print






")









