


Introduction
Chronic kidney disease (CKD) is characterized by kidney structure or function abnormalities that are present for >3 months. The prevalence of CKD is 14.8% in adults in the United States [1] and 6% to 26% in Europe [2]. About 280 patients with end-stage renal disease (ESRD) in one million people need hemodialysis or peritoneal dialysis [3]. As short-term mortality in most patients with ESRD on hemodialysis continues to decrease due to improvements in dialysis technology, the increase in life expectancy has been accompanied by a burden of morbidity in later life [3]. Older patients on maintenance hemodialysis (MHD), in the same way as in the general population of older people, suffer from greater impairments of sensory and motor functions relating to aging, which reduces the quality of life and increases dependency [4].
Over 5% of the world’s population suffers from hearing loss (HL), one of the most common sensory disabilities with normal aging [5]. Hearing difficulties in older adults are undertreated, resulting in several adverse consequences such as decreased communication and reduced quality of life [6,7], including social withdrawal, anxiety, depression, and loss of confidence [8]. These adverse consequences and HL have been significantly related to cognitive impairment and independence in the older population [9]. Still, HL is manageable with hearing aids and even surgery [10].
Physical performance is an important health factor for patients undergoing hemodialysis and in the general population of older adults. With age, physical performance (such as balance, walking speed, and muscle strength) gradually decreases, leading to a high risk of falls [11] and subsequent fractures [12], hospitalizations, loss of independence, and even increased mortality [13,14]. Poor physical performance is also related to other serious problems, including cognitive deterioration and the inability to maintain health-related quality of life [11]. Good physical function and performance are essential to prevent various health conditions and immobility in the elderly [15], and exercise could improve frailty and quality of life among hemodialysis patients [16]. Therefore, it is vital to identify modifiable risk factors for diminished physical performance in patients on MHD because targeted interventions may ameliorate these outcomes.
HL is an overlooked potentially modifiable risk factor for poor physical performance in patients with MHD. A few previous studies examined the associations between HL and physical function and performance in other populations, but the results were inconsistent [17–20]. Whether there is a correlation between HL and physical performance in patients on MHD has not been investigated. Therefore, the present study aimed to explore the association between HL and physical performance.
Methods
Study design and population
This multicenter cross-sectional study was conducted between July 2020 and April 2021 in seven outpatient hemodialysis centers in Shanghai and Suzhou, China. The study was approved by the Ethics Committee of Shanghai Fifth People’s Hospital &(No. 2020-182). The methods were carried out in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment in the study.
The inclusion criteria were 1) ≥18 years of age, 2) received MHD for at least 3 months, and 3) able to provide informed consent. The exclusion criteria were 1) unable to communicate with interviewers due to dementia, mental illness, or other neurodegenerative diseases, 2) ear infection, cochlear implant, or hearing aids, 3) assessed by the investigator as unable to complete all performance-based tests due to severe disability, 4) acute infection, pulmonary edema, acute cardiovascular disease (acute coronary syndrome or arrhythmia), acute cerebrovascular disease (infarct, hemorrhage), amputated limb, or malignancy, or 5) refused to provide informed consent.
Hearing assessment
The hearing assessment was performed using pure-tone audiometry (BTJ09; Jiangsu Better Life Medical Co., Ltd, China) by trained examiners in a sound-isolated room. Air conduction hearing thresholds were recorded, which were measured for each ear at different frequencies (0.125, 0.25, 0.5, 0.75, 1, 1.5, 2, 3, 4, 5, 6, and 8 kHz) and across an intensity range of 0 to 100 decibels (dB). The speech frequency pure-tone average (PTA) was calculated as the mean thresholds across 0.5, 1, 2, and 4 kHz [19]. HL was defined as a PTA ≥ 25 dB, reflecting mild to profound HL according to the American Speech-Language-Hearing Association [21], which was used as a cutoff point in either ear in the present study [19, 22].
Physical performance
The physical performance included balance function, muscle strength, and mobility measured using the Timed Up and Go Test (TUGT), handgrip strength, and gait speed, respectively. The TUGT involved getting up from a chair, walking for 3 m, turning around, walking back to the chair, and then sitting down again with back against the chair [23]. Handgrip strength assessment was performed on the non-fistula hand or the dominant hand of the patients with an indwelling dialysis catheter, using a dynamometer (GRIP-D; Takei Ltd.). The participants were asked to exert maximum effort twice, and the best of two measurements was registered [24, 25]. Gait speed was assessed with the 4-m walk test. Walking aids were allowed during the test [23]. These tests were performed before a hemodialysis session.
Data collection
The demographic and clinical data were collected, including age, sex, body mass index (BMI), dialysis vintage, cause of ESRD, education, drinking, smoking, Charlson comorbidity index (CCI), living alone, fall, and laboratory parameters such as hemoglobin, serum albumin, and fractional urea removal rate (Kt/V).
Statistical analysis
Data were presented as means ± standard deviations or medians (interquartile range) for continuous variables and as number (%) for categorical variables. Comparisons were performed using a t test for the continuous variables and a chi-square test for the categorical variables. The Spearman correlation coefficient was used to assess the correlations of the PTA with physical performance. A trend test was used to detect the increased prevalence of HL using the Cochran-Armitage test among three groups (aged <60, 60–74, and ≥75 years). Logistic regression analysis was used to investigate the relationship between HL and TUGT, handgrip strength, and gait speed in all enrolls and across different age groups. We then calculated odds ratios (ORs) and 95% confidence intervals (CIs) according to the quartiles of TUGT, handgrip strength, and gait speed when covariates were added sequentially to the logistic model. Crude was the unadjusted model. Model 1 was adjusted for age and sex. Model 2 was adjusted for Model 1 variables and BMI, CCI, education, smoking, drinking, fall, and serum albumin. The interaction effect between the component of physical performance and age was tested by adding three interacted items (TUGT × age; handgrip strength × age; and gait speed × age) in the logistic regression analysis. All statistical analyses were performed using IBM SPSS version 26.0 (IBM Corp.). A two-sided p-value of <0.05 was considered to be statistically significant.
Results
Clinical characteristics
This study included 880 patients on MHD, but the final sample consisted of 838 patients (male, 516) after excluding 20 patients who refused to participate in the hearing assessment, two who did not complete the handgrip strength test, and 20 who did not complete the TUGT or gait speed test (Fig. 1). Of the 838 participants (mean age, 61.2 ± 12.6 years), 516 (61.6%) were male, and 423 (50.5%) had mild to profound HL in at least one ear (male, 48.6% and female, 53.4%). The mean age of the individuals with and without HL were 67.0 ± 10.3 and 55.3 ± 11.9 years, respectively (p < 0.001). The patients’ socioeconomic and health-related characteristics according to their hearing status are presented in Table 1. Compared with those without HL, participants with HL were less educated (p < 0.001) and had a higher CCI (p < 0.001), lower serum albumin levels (p = 0.003), and a history of more frequent falls in the previous year (p = 0.011).
Association between hearing thresholds and physical performance
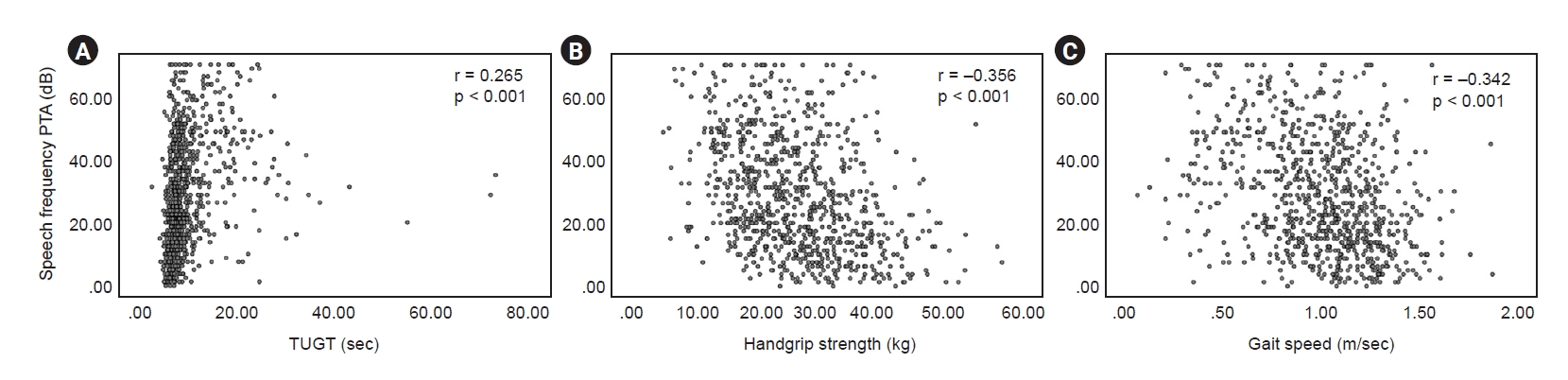
Patients with HL had a significantly weaker handgrip strength, slower TUGT, and gait speed than subjects without HL (all p < 0.001) (Table 1). TUGT was positively correlated with PTA (r = 0.256, p < 0.001). Handgrip strength and gait speed were negatively correlated with PTA (r = –0.356, p < 0.001 and r = –0.342, p < 0.001, respectively) (Fig. 2).
Table 2 presents the ORs of HL for physical performance measures when the participants were divided into four groups by quartiles based on TUGT, handgrip, and gait speed. In the unadjusted model and model 1 (adjusted for age and sex), HL was associated with a slower TUGT (p for trend = 0.001 and p for trend = 0.004, respectively). The result still held true after adjusting for all covariates (p for trend = 0.005). In this final model, the OR for HL was 1.15 (95% CI, 0.73–1.81) for the second fastest quartile of TUGT, 1.69 (95% CI, 1.07–2.70) for the second slowest quartile of TUGT, and 2.87 (95% CI, 1.69–4.88) for the slowest TUGT quartile, compared with the fastest TUGT quartile. A similar trend was also observed for handgrip strength in the unadjusted and adjusted groups (models 1 and 2) (p for trend = 0.048, p for trend = 0.043, and p for trend = 0.045, respectively). In the final model, the multivariable-adjusted ORs for HL across handgrip strength (lowest to highest) were 1.00 (reference), 0.61 (95% CI, 0.39–0.97), 0.46 (95% CI, 0.28–0.76), and 0.31 (95% CI, 0.17–0.56). There were no associations between HL and gait speed in the unadjusted model and after adjustments for all covariates; however, a trend persisted (p for trend = 0.06 and p for trend = 0.05, respectively).
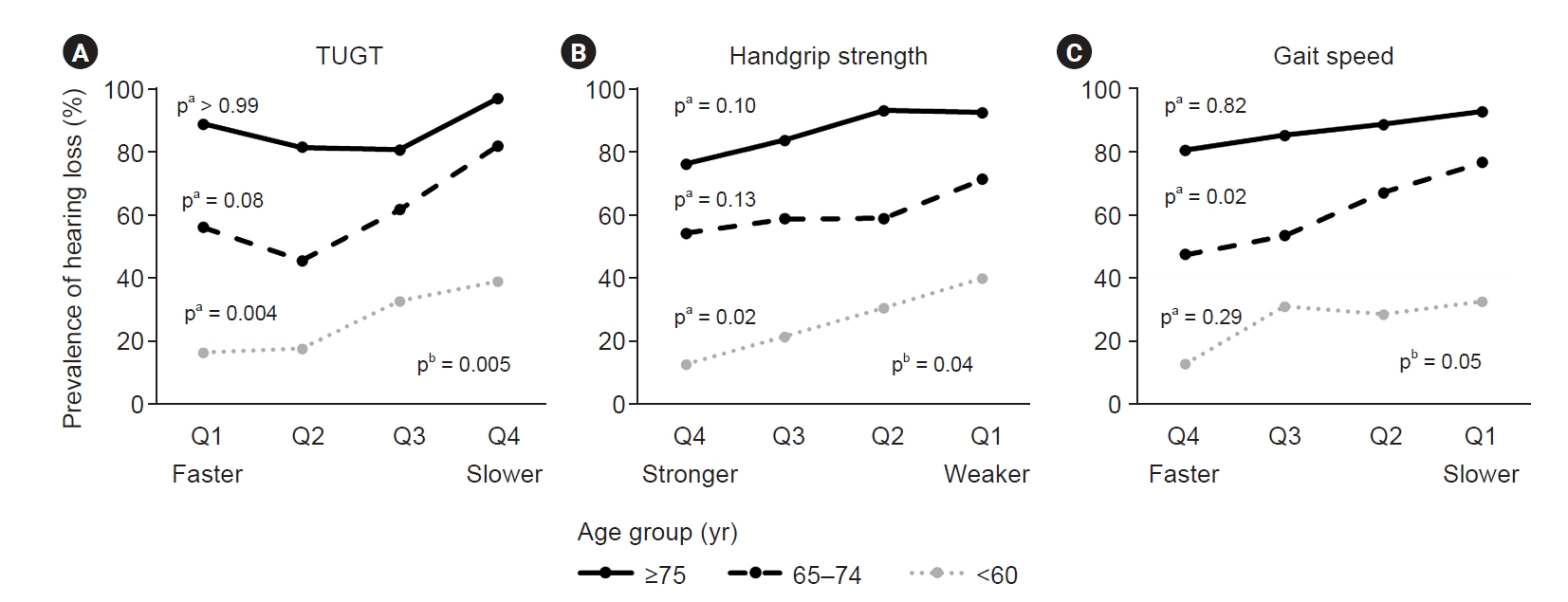
Fig. 3 shows that the prevalence of HL in patients aged ≥75, 60 to 74, and <60 years was 86.1%, 60.9%, and 26.7%, respectively. In the <60 years group, TUGT exhibited a significant dose-response relationship with HL (p = 0.004). This trend was also detected in the 60 to 74 years group (p = 0.082), while similar relationships were not observed in the aged ≥75 years group (p > 0.05). This outcome was supported by our findings that there was a significant interactive effect of age on the relationships between HL and TUGT (p for interaction < 0.001). Additionally, handgrip strength showed a noteworthy dose-response relationship with HL only among individuals aged <60 years group (p = 0.02). A similar relationship between HL and gait speed was detected only among those aged 60 to 74 years (p = 0.02) (Table 3–5, Fig. 3).
Discussion
This study indicates that mild to profound HL at speech frequency PTA in either ear was associated with a slower TUGT and a weaker handgrip strength after adjustment for sociodemographic and lifestyle characteristics, comorbidities, falls, and serum albumin. The findings provide basic epidemiological data on HL in patients on MHD in China, as well as data comparing the physical performance according to the hearing status.
This population-based study of patients on MHD showed that 423 of the 838 participants (50.5%) had a certain degree of HL in at least one ear. Moreover, it is well known that patients on MHD often have comorbidities, including diabetes, hypertension, and cardiovascular diseases [26]. Previous studies argued that these chronic diseases were related to HL [27,28]. Our findings demonstrated a level of statistical significance in the association between PTA and physical performance. Despite relatively modest correlations, the results provide important clues for early evaluations that emphasize hearing and performance.
Regarding the relationship between HL and TUGT, the present study was consistent with Yévenes-Briones et al. [29] using data from the Seniors-ENRICA (Study on Nutrition and Cardiovascular Risk in Spain)-2 study, who observed that difficulty in rising from a chair and balance impairment were associated with HL. Although the definition of HL was different from the present study, it did not affect the consistency of the conclusions between the two studies. The results were also consistent with Bang et al.’s [30]. Their cross-sectional study indicated that postural instability was associated with HL. Furthermore, a prospective study revealed that both mild and moderate or greater hearing impairment were correlated with a lower Short-Physical Performance Battery (SPPB) [31]. The longitudinal analyses by Martinez-Amezcua et al. [19] demonstrated that compared with participants with normal hearing, those with HL had a faster decline in physical function over time. In another study, Martinez-Amezcua et al. [20] concluded that balance was independently related to hearing impairment. Furthermore, our research uncovered that age acted as an effect modifier for the correlations between HL and TUGT, then age-specific evaluations and interventions focusing on the physical performance and auditory function ought to be conducted. On the other hand, Goins et al. [17] found that all individual SPPB component scores had no relation to HL, where audiometry was based on self-reported measurements. Mueller-Schotte et al. [18] showed that the number of instrumental activities of daily living limitations was not higher in self-reported HL compared with no sensory loss. This heterogeneity may be explained by the difference in audiometry (subjective self-report vs. objective clinical audiometry).
The present study showed that the gait speed was 1.0 ± 0.3 m/sec, which was lower than that of older adults in communities and similar to the data of 277 patients on MHD obtained by Lee et al. [32]. In older Japanese people, the gait speed was 1.2 ± 0.2 m/sec [33]. In Chinese community-dwelling older adults, the gait speed was 1.1 ± 0.2 m/sec [23]. Ozawa et al. [34] confirmed that the gait speed was significantly declined in elderly patients with heart failure. Another study showed that poor glycemic control was significantly correlated with the decrease in gait speed in Japanese patients with type 2 diabetes [35]. The high prevalence of sarcopenia in patients on MHD (40%) can have a negative impact on handgrip strength and gait speed [24].
Yévenes-Briones et al. [29] indicated that the chair stand test was significantly associated with hearing impairment but not gait speed, while other studies showed that gait speed was independently associated with hearing impairment [20,36]. Chen et al. [31] also reported that during a 10-year long-term follow-up, the participants with greater hearing impairment had slower gait speeds. The present study revealed that the correlation between HL and a slower gait speed nearly reached statistical significance, but further study is needed to explore the mechanisms of this relation.
HL was associated with worse physical activity [37] and was a risk factor for disability in older individuals [38]. Previous studies examined the associations between HL and frailty syndrome and disability [9,18,29,31,38], and their results were consistent. Interestingly, the present study revealed an association between HL and handgrip strength, consistent with Kim et al. [25], who concluded that both moderate and impaired self-reported hearing acuity of the 3,075 participants were significantly associated with weak handgrip strength. In contrast, Tomioka et al. [36] reported no significant association between self-perceived hearing handicap and handgrip strength in high-functioning older adults. Another prospective cohort study showed no significant negative correlation between handgrip strength and unilateral and bilateral HL development [39]. Therefore, whether grip strength can be used as an early warning signal of HL or hearing is beneficial to grip strength requires confirmation in other settings and additional investigation.
This study had some limitations. First, the cross-sectional design made it impossible to assess causal relationships between HL and physical performance, but only associations. Second, the hemodialysis centers of the seven hospitals did not randomly select the participants. Therefore, the samples might not be representative of the entire hemodialysis population. Third, not all patients were consecutively included but voluntarily participated. Thus, the patients not in the study might have more severe physical performance decline and/or HL or different socioeconomic characteristics, which might lead to bias. Fourth, our study did not analysis those dialysis related factors such as dialysis type (high flux, low flux, and hemodiafiltration), dialysis time, and frequency of dialysis, and the impact of these differences may have been overlooked. Despite these limitations, to the best of the authors’ knowledge, this work addressed the knowledge gap about the relationship between HL and physical performance in patients with MHD. In addition, multicenter prospective studies with larger sample sizes, such as randomized controlled trial, remain to be needed in the future.
In conclusion, the present study suggests that a faster TUGT and a stronger handgrip strength are associated with a lower prevalence of HL in patients with MHD. Recognizing these associations could lead to earlier hearing- and performance-based assessments with appropriate interventions.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









